All published articles of this journal are available on ScienceDirect.

Towards a Dynamic Assessment of Unilateral Spatial Neglect
Authors Info & Affiliations
Abstract
Background:
The traditional paper and pencil tests are often inadequate to detect the mild forms of Unilateral Spatial Neglect (USN).
Objective:
To verify the effectiveness of a touchscreen-based cancellation test in assessing individuals with USN.
Methods:
Seven individuals, six with right and one with left brain damage, who showed moderate to severe USN at admission, were involved in the study. Besides classic paper and pencil tests, participants were presented with a new, “user-friendly”, device consisting of an interactive “table” that integrates the principles of ecologic interaction and sophisticated technology. Such a touch screen table made possible to analyse the spatial and temporal evolution of the participants’ performance, providing a set of indices related to “how” the different tasks have been fulfilled, rather than simple raw scores.
Results:
This new technological approach turned out to be much more sensitive than the classic paper and pencil tests to detect the slightest forms of USN. In particular, while four out of the seven participants, performed flawless on the papery version of the Albert’s test, all of them made errors on the technological versions of the same Albert’s test. Finally, under all the different experimental conditions, participants achieved always a better performance when asked to erase rather than mark stimuli.
Conclusion:
Such a device has a potential in the ecological assessment of USN as well as in monitoring its evolution. Although in need of further substantiation, our findings further support the need to go beyond the traditional paper and pencil tests in the assessment of USN. The information provided by a more dynamic approach seems to be relevant for both clinical and research purposes.
INTRODUCTION
The unilateral spatial neglect (USN) is a neuropsychological syndrome characterized by the inability to orient to, act upon, and perceive stimuli delivered to the contralesional part of the space [1]. As a consequence, individuals affected by USN behave as though their extrapersonal and personal spaces contralateral to the lesion are absent, and they seem to “exist in a demi-world where laterality determined reality” [2].
Typically, symptoms tend to abate in weeks to months, and most individuals show a full recovery within 3 months after onset. However, approximately 10% of them still show signs of severe USN 6 months after onset and longer, and are diagnosed as having chronic USN [3]. Despite the fact that language, memory and other cognitive abilities are comparatively spared, persistent USN predicts a poor outcome and markedly reduces the possibility of independent living while increasing potential of painful injury. In summary, persistent USN is the worst prognostic factor for recovery in hemiplegia [4, 5].
The above emphasizes the importance of an accurate and early diagnosis leading to an optimal treatment of USN syndrome. Unfortunately, USN is often misunderstood and many cases of USN go undetected. Indeed, USN syndrome is not well known outside the small circle of neurologists and neuropsychologists so that many physicians still ignore its existence, and do not assess its presence. Moreover, even when investigated, many cases of USN are not recognized, because a lack of sensitivity of the tests used to assess it. In this scenario, it is evident the need to go beyond the traditional paper and pencil tests which are often inadequate to detect mild to moderate USN.
The paper and pencil tests allow to easily compute the incidence and spatial distribution of omissions. Further, the time taken to perform these tests can certainly give additional, useful, information. Raw scores and time, however, are purely static data that offer only an approximate idea of the way individuals with brain-damage (BD) analyse the space around them. Thus, a more dynamic approach seems ineluctable. In particular, the strategy used to accomplish the given task has great potential to disclose the mechanisms underlying the spatial information processing in individuals with BD.
In the recent years, the development of digital technology made possible to build up sophisticated devices that allow the registration of the various parameters underlying the participants’ behavioural performance. Most of these devices approaches are based on virtual reality (VR) or augmented reality environment, and give the opportunity to evaluate participants with ecological paradigms that look like daily activities. Nowadays, the VR technology is widely used in experimental studies because while it provides the participant with a safe and friendly-user context, it allows the examiner to precisely control the variables involved in the experiment. Thus, not surprisingly, many devices have been developed to serve both research and clinical purposes [6-9].
Among the several methods employed to assess USN, such as figure copying, line bisection, reading and writing tasks, the most common ones are the various types of target cancellation tests [10]. Irrespective of the specific features peculiar to each of them, all the cancellation tests require participants to cancel out targets interspersed with distractors and arranged in a display located in front of the participant, aligned with his/her mid-sagittal plane body. An elevated or at least a greater number of stimuli omitted in the contralesional than ipsilesional side of space is considered as a hallmark of USN [11].
The first computerized version of a cancellation task dates back to the end of the last century [12]. Since then, several computerized cancellation tasks have been proposed [6] to examine the individuals’ (with or without USN) performance in a virtual environment.
Overall findings are consistent to support the notion that computerized testing is as, or even more, sensitive than classic pencil and paper tests to assess USN. Furthermore, the computerized assessment has potential to provide, beside a reliable measure of cancellation performance, a sensitive measure of search organisation. In this vein, several studies demonstrated that individuals with USN have an inescapable tendency to explore and re-explore ipsilesional locations and mark and re-mark the targets (i.e. perseveration) failing to keep track of them during search [13, 14].
Moreover, even after having recovered from USN, these individuals showed a mixed (i.e. neither horizontal nor vertical) search pattern, repeated target pressures and deviating hand movements [15-17].
Rabuffetti, Farina, Alberoni, Pellegatta, Appollonio, Affanni, et al. [18] implemented a computerized cancellation test adopting a touch screen interface. Stimuli were letters or shapes. Along with classic indices (i.e. the number of targets detected), the device allowed authors to evaluate other interesting parameters such as the number of perseverations, the latency (i.e. the time elapsing between two detections) and the search speed.
As said before, however, no single test taken in isolation can satisfy the need of an accurate assessment of USN. In this vein, Azouvi, Samuel, Louis-Dreyfu, Bernati, Bartolomeo, Beis et al. [19] reported that USN incidence increases from 50% to 85% of individuals with right brain damage (RBD) when the assessment was based on several rather than one single paper and pencil test. Bearing this in mind, Fordell, Bodin, Butch, and Malm [20] developed a Visual Reality Diagnostic test battery aimed to evaluate different cognitive domains that are likely to be affected in individuals with USN. The battery test reached 100% of sensitivity and 82% of specificity in accurately identifying cases of USN.
Thus, technology can provide examiners with accessible and reliable methods to assess the degree of USN in individuals with BD. The further step is to develop diagnostic tools that do not stray much from the operations performed daily by the individuals with BD. In other words, there is a propensity to use technology to simulate naturalistic environments.
Here we set out to address these issues by means of a novel application in neglect assessment based on cancellation tasks in a virtual, daily living, environment. Seven individuals, six with right and one with left brain damage (LBD), with clear signs of USN on hospital admission, were examined. The experimental tests allowed us to explore: a) whether the technological assessment is more sensitive than the classic paper and pencil tests in detecting residual USN; namely, whether the sole dynamic information provided by technological tool is reliable enough to allow a proper evaluation of USN participants’ performance; b) whether, also in a virtual environment, the performance of participants with USN differs depending on the type of task; namely, whether the eraser procedure which is thought to reduce attentional bias [21] is less severely impaired than the classic marking procedure.
METHODS
Participants
One female with LBD and six (4 female) individuals with RBD ranging in age from 62 to 81 years recruited form a series of consecutive referrals to the hospital on the basis they met the inclusion criteria (see below), verbally volunteered to be enrolled in the study which was approved by a departmental ethics committee and carried out in accordance with the guidelines of the Declaration of Helsinki. Seven healthy people matched 1:1 for age and education with the study group gave an informed consent to serve as control group. All participants and controls had normal or corrected to normal visual acuity and no visual field defects, good comprehension and were naïve as to the research purpose. All participants with BD underwent a rehabilitation training lasting about three months.
At both admission and discharge, the presence and severity of USN was assessed in each participant by means of six different tests, including two cancellation tests (i.e. bell cancellation test [22], Albert’s test [23]), a sentence reading test [24], and a copying, a drawing, and a line bisection test [25].
In the Bell cancellation test [22] participants were requested to cross out a designated target (i.e. bell) randomly interspersed among many other items with an equal number of targets lying to the left and to the right of the paper.
The Albert’s test [23] consisted of a series of seven columns of black lines that participants had to cancel. Three of the seven columns were on the left side, three on the right, and one in the centre of an A4 sheet of paper horizontally arranged, for a total of 24 target lines.
In the sentence reading test [24] participants were to read aloud three sentences written in capital letters, and presented one by one aligned horizontally in the centre of a sheet of paper so that an equal number of syllables lied to the left and to the right.
In the copying test [25] participants had to copy three b/w symmetrical drawings (i.e. a house, a star, a daisy) presented one by one at the centre of a paper sheet. Due to its symmetrical structure, each drawing had an equal number of line segments lying to the left and to the right (as well as some segments lying in the centre).
In the drawing test [25] participants were requested for two free drawings of a clock face with numbered dials and hands pointing towards 10:10 and 9:15, respectively.
On all the above tests, the participants’ performance was scored for rate of contralesional omissions (or displacements in the case of the copying, and drawing tests). For each test, an arbitrary cut-off point was drawn to distinguish two levels of impaired performance. According to the rules suggested by Gainotti, D’Erme, and Bartolomeo [26] a rate of more than 40% of contralesional omissions (or displacement of more than 40% of the lateralised subcomponent of the figure or text in the drawing, and copying test, respectively) was taken as an index of severe USN, whereas performances with less than 40% of contralesional omissions (or displacements) were judged as indicative of mild/moderate neglect.
Finally, in the line bisection test [25] participants had to indicate the midpoint of a series of lines of various length. For each line the distance between the actual (i.e. the point at which participant placed the midpoint) and the expected (i.e. the true midpoint) was taken as a measure of the progressive shift towards the side of the lesion typically observed in individuals suffering from USN. Consistently with the rules suggested by Gainotti et al. [26], we considered a shifting of the actual midpoint [mean value: S of the shifts / number of the lines (i.e. six)] exceeding 20% of line length as an index of severe USN.
Following these criteria, the participants’ performance in each test was scored on a three-points scale ranging from 0 to 2:0 indicated a correct performance, 1 and 2 a mild/moderate and a severe impairment, respectively. Thus, for each participant an overall neglect severity score (NSS) ranging from 0 (no deficit) to 12 (severe deficit in all the tests), was computed.
Inclusion criteria were: a) having suffered unilateral, vascular, brain damage; b) the absence of a general cognitive impairment (i.e. MMSE [27] score above the cut-off); c) an overall level of motor functioning that could allow participants with BD to perform the technological tasks; d) an overall NSS at admission ranging from 7 to 12, indicating a severe neglect; e) an overall NSS at discharge ranging from 0 to 1, indicating a substantial recovery from USN.
Control participants were examined in a single session. Needless to say, they performed at ceiling on all the tests for the assessment of USN.
Stimuli and Procedure
The interactive table was developed by the MICC - Media Integration and Communication Centre of the University of Florence. It combines the principles of ecologic interaction with the high-tech devices, and represents the new frontiers in the assessment and rehabilitation of individuals with USN. In particular, this table device is provided with a 52 multi touch screen monitor similar in shape to a dinner table with a wood surface-like.
A uniform distribution of stain images was displayed on the top which varied for number: 24 or 48, and nature: coffee or water stains, and dust grains. Participants were to detect and cancel the stains by using a round sponge.
For each stimulus, the examiner could choose location, size and nature. Since our main aim was to compare the participants’ performance on the classic Albert’s test with that on the same Albert’s test carried out on the interactive table, the stimuli were arranged to reproduce the stimuli size and disposition in the papery Albert’s test. Moreover, each stain cancellation was carried out under two conditions: a more ecologic one in which as the sponge touched the spot it disappeared, and the other more similar to the classic Albert’s test in which as the sponge touched the spot it was marked by a red line.
Each participant was involved in three experimental conditions, carried out in this fixed order with a short rest period between them: 1) 24 coffee stains; 2) 48 coffee stains; both performed under the two cancellation modalities described above and the order of which was counterbalanced across participants; 3) dust grains.
All the experimental sessions were conducted in a dimly lit and quiet room. Participants were seated in front of the device, centrally oriented. The table was 45° tilted, so that even the participants with reduced mobility could arrive to every point on the table. No time limit was imposed and the participants were assessed to the limit of their possibilities. However, according to the rules suggested by Rabuffetti et al. [18], if a participant had not declared the test conclusion after 10 minutes, he/she was asked whether the test was finished or not.
RESULTS
As expected, healthy controls performed errorless in all experimental conditions, so only their time data along with their cancellation pattern were used as benchmark for comparison with the performance of participants with BD as is shown in detail in Tables (1 and 2).
| Stains 24 Albert like | Stains 24 Eraser | Stains 48 Albert like | Stains 48 Eraser | Dust | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Patient | Albert's | Acc. | Time | Acc. | Time | Acc. | Time | Acc. | Time | Acc. | Time | ||||||||||
| paper | |||||||||||||||||||||
| RBD 1 | 100% | 20.8% | 160” | 75% | 162” | 81.8% | 212” | 74.8% | 224” | 52% | 92” | ||||||||||
| RBD 2 | 100% | 75% | 29” | 100% | 18” | 58.2% | 29” | 97.2% | 72” | 70% | 27” | ||||||||||
| RBD 3 | 100% | 95.8% | 62” | 100% | 33” | 67.8% | 149” | 100% | 118” | 94% | 463” | ||||||||||
| RBD 4 | 82.5% | 95.8% | 33” | 100% | 26” | 31.8% | 37” | 100% | 46” | 99% | 108” | ||||||||||
| RBD 5 | 100% | 95.8% | 101” | 83,3% | 75” | 83,3% | 220” | 79,2% | 132” | 70% | 268” | ||||||||||
| RBD 6 | 15% | 16,7% | 30” | 25% | 27” | 16,5% | 53” | 30,3% | 59” | 13% | 19” | ||||||||||
| LBD 1 | 70% | 33,3% | 54” | 54,2% | 58” | 33,2% | 192” | 49.8% | 161” | 37% | 104” | ||||||||||
| Controls | |||||||||||||||||||||
| mean value | 100% | n.p. | n.p. | n.p. | n.p. | 100% | 17.4 | 100% | 18.2 | 100% | 35.4 | ||||||||||
| sd | = | = | 6.7 | = | 3.5 | = | 2.1 | ||||||||||||||
| Stains 24 Albert like | Stains 24 Eraser | Stains 48 Albert like | Stains 48 Eraser | Dust | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Subject | Albert's | Acc. | Time | Acc. | Time | Acc. | Time | Acc. | Time | Acc. | Time | ||||||||||
| paper | |||||||||||||||||||||
| RBD 1 | 100% | 100% | 80” | 100% | 44” | 100% | 74” | 100% | 48” | 100% | 232” | ||||||||||
| RBD 2 | 100% | 100% | 16” | 100% | 19” | 97.2% | 31” | 100% | 26” | 100% | 46” | ||||||||||
| RBD 3 | 100% | 100% | 45” | 100% | 22” | 55.3% | 89” | 61% | 39” | 100% | 108” | ||||||||||
| RBD 4 | 100% | 100% | 19” | 100% | 16” | 100% | 34” | 100% | 26” | 100% | 49” | ||||||||||
| RBD 5 | 100% | 100% | 26” | 100% | 18” | 98.5% | 52” | 100% | 28” | 100% | 67” | ||||||||||
| RBD 6 | 100% | 50% | 80” | 58,3% | 38” | 44,2% | 87” | 65% | 72” | 49% | 89” | ||||||||||
| LBD 1 | 100% | 95.8% | 61” | 100% | 21” | 97% | 104” | 100% | 51” | 100% | 145” | ||||||||||
| Controls | |||||||||||||||||||||
| mean value | 100% | n.p. | n.p. | n.p. | n.p. | 100% | 17.4 | 100% | 18.2 | 100% | 35.4 | ||||||||||
| sd | = | = | 6.7 | = | 3.5 | = | 2.1 | ||||||||||||||
Data Analysis
Given the large variability usually found in individuals with BD and, in particular in those with neglect, following the suggestion of a recent paper in the field of neglect rehabilitation [28], we analysed the data from participants with BD as a group as it concerns the parameter accuracy and as multiple single cases as it concerns the parameter time taken to perform the task.
Accuracy. From a qualitative point of view, as to the admission evaluation, it is worth noting that, while four participants with RBD, made no errors in the papery version of the Albert’s cancellation test, all of them made errors (see Table 1 for details) when performing the more demanding table tasks, in particular the marking version. In turn, as to the discharge evaluation, the main result was that all participants made very few errors if any on all the experimental tests (see Table 2 for details). Once again, however, for both the 24 and 48 stains stimuli tasks, accuracy was higher when participants were requested to erase than mark. However, with the aim to investigate whether the participants with BD’s performance on the table tasks varied throughout the period of study, according to the cancellation modality requested, and the number of stimuli, for each member of the experimental group the performance on the different tasks (i.e. marking vs erasing procedure) with different number of stimuli (i.e. 24 vs 48) at the different periods (i.e. admission vs discharge) was entered into a repeated measures ANOVA with period, task and number of stimuli as the within-subjects factors.
Results were straightforward. The main factors Period [F (1,6) = 8,2, p = .003] turned out to be significant because participants’ performance improved markedly from pre to post-training period. Analogously, the main factor Task [F (1,6) = 16,85 p = .006] was significant as well due to the fact that participants were more accurate when requested to erase than mark. The interaction Period by Task tended to significance [F(1,6) =5.85, p = .052] because participants’ improvement was more evident in the Albert than in the eraser task.
Time: The participants’ amelioration across period of testing was even more evident when the parameter time was considered. Moreover, all participants performed faster when requested to erase than mark, albeit this difference reached statistical significance only on the more demanding 48 items condition (paired t-test: p = 0.032), but not in the 24 items condition (paired t-test: p = 0.107). Even the fastest participants with BD, however, performed at least 2 SD slower than the control mean and almost all these differences turned out to be statistically significant (Crawford-Howell t-test for case-control comparison: p values ranged from 0.0001 to 0.025).
Although interesting, accuracy and time taken to carry out the various tests failed to provide relevant information of the way participants with BD explore their extra-personal space. For this purpose, it could be very relevant to examine the dynamic data provided by the table.
Consistent with recent findings from a large sample of healthy adults [29], control participants showed a typical reading like (i.e. horizontal left to right) search pattern.
In turn, in line with the large variability usually found in individuals with USN [30, 31] the search patterns expressed by participants with BD were much more various (see Fig. 1). Typically, however, even when they performed the task without errors and in a relatively short time, participants with BD tended to start their search from the ipsilesional side of the table and explore the contralesional part of the array only after having marked (erased) all the stimuli on the ipsilesional space (see Fig. 2).
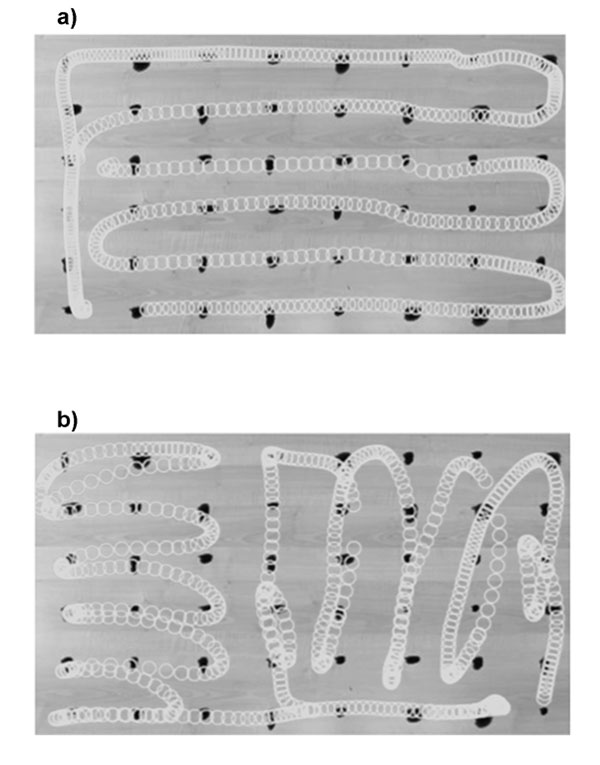
Legend: a) Example of control participants’: Typical search pattern b) Example of BD patients’ search pattern.
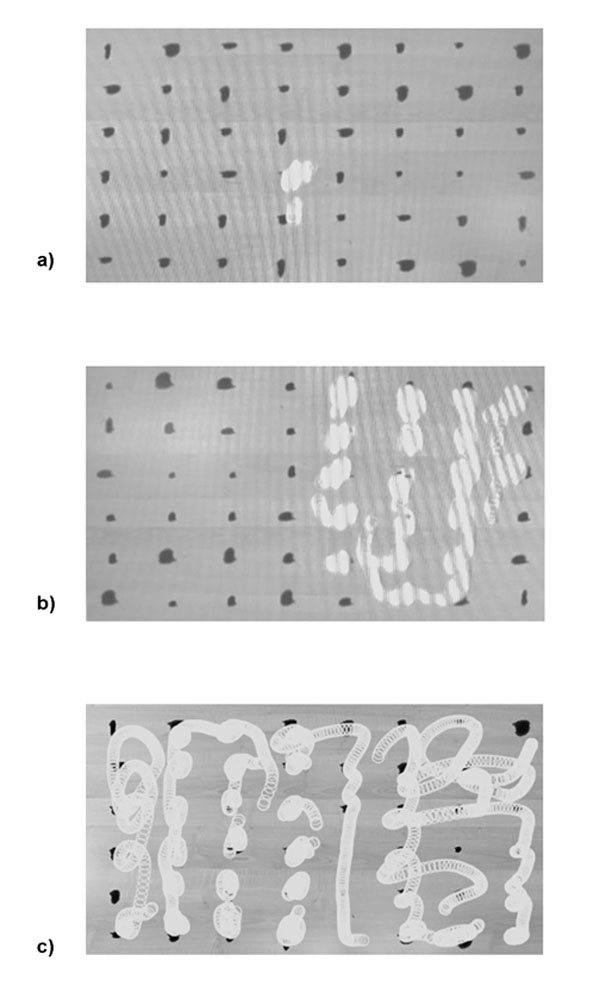
Legend: a) Starting point; b) Half performance; c) Final output.
Finally, consistent with previous studies on participants with USN [13, 14], we also observed several perseverations (i.e. participants tended to mark and mark again rightward locations) which were much more frequent when they were requested to mark than erase.
DISCUSSION
This research mainly aimed to demonstrate that the technological version of the classic cancellation tests is more sensitive than the classic paper and pencil tests to detect the slightest forms of USN.
To address this issue, we selected a series of six individuals with RBD and one with LBD who based on standard clinical criteria have been diagnosed as having a severe USN at hospital admission. All of them received motor and cognitive rehabilitation at the end of which they were diagnosed as having substantially recovered from USN.
At both admission and discharge, besides classic paper and pencil tests, participants were also requested to carry out different technological versions of cancellation tests. The comparison of participants’ performance in papery and technological version of cancellation tests, gave very interesting results (see Table 1 and 2).
First, the interactive table has proven to be a more sensitive tool than the traditional papery tests. In particular, it is worth noting that on admission, four out of the seven participants, performed flawless on the papery version of the Albert’s test. Thus, a diagnosis of USN has been possible only by administering these participants with a complete battery of paper and pencil tests. In turn, all participants made errors on the technological versions of the same Albert’s test, especially on the more demanding 48 stimuli version and even in a higher degree on the “dust” task. That is, the sole participants’ performance on this task could have allowed a diagnosis of USN. To sum up, the interactive table has potential to become a first choice test for the diagnosis of USN, even its slightest forms.
Interestingly, participants achieved always a better performance when asked to erase rather than mark stimuli. This result is consistent with the Kinsbourne’s claim [32] that a right hemisphere lesion leads to a rightward orienting bias which is too strong to be compensated by the intact left hemisphere. The fact that in our tasks the number of left sided omissions decreased by having participants to erase rather than mark is explained by assuming that right sided visual stimuli have a such magnetic power to drive participants’ behaviour, unless left sided visual stimuli are more relevant. While the classic Albert’s procedure leaves right sided stimuli intact, the eraser procedure removes the right-sided stimuli, thus reducing the attentional bias [21].
A last point deserves comments. On discharge, all the participants with BD were diagnosed as USN-free on standard clinical criteria. Analogously, when examined with the interactive table, these participants were very accurate and only slower than healthy controls. Thus, one could argue that the more cumbersome and expensive technological tool is as sensitive as the infinitely simpler and cheaper battery of paper and pencil tests. That should be true if only static data as raw score and time taken to accomplish the task were considered. The interactive table, however, besides static data can also provide dynamic data which turned out to be a very important parameter to understand the way participants with BD explore the space around them. As shown in Figs. (1 and 2), although participants with BD’ performance was indistinguishable from that of healthy controls on a quantitative point of view, participants with BD demonstrated a quite disorganized pattern of exploration, strongly different from the typical reading pattern usually observed in literate people. This finding is consistent with recent evidence from a large sample of participants with BD demonstrating that compared to healthy people, participants with BD either left or right show a disorganized search, even more evident in those of them with USN. However, unlike what found by Ten Brink, Van der Stigchel, Visser-Meily, and Nijboer [33] we did not find any clear difference between participants with right and left BD (only one), so we can claim that, irrespective of the lesioned hemisphere, even participants with BD diagnosed as USN-free based on standard clinical criteria, may show residual evidence of USN when assessed on a more challenging test (and a more sensitive parameter is considered).
CONCLUSION
In conclusion, our findings further support the need to go beyond the traditional paper and pencil tests in the assessment of USN. The information provided by a more dynamic approach, although in need of further substantiation, seems to be relevant for both clinical and research purposes.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
No Animals/Humans were used for studies that are base of this research.
CONSENT FOR PUBLICATION
Not applicable.
CONFLICT OF INTEREST
The author confirms that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
We are grateful to the participants with BD who took part in the experiment for their kind co-operation. The financial contribution of the MIUR, Italy, is also gratefully acknowledged.

