All published articles of this journal are available on ScienceDirect.

Attitudes Towards Procreative Options in the Event of Infertility: The Role of Personal Values and Religiosity
Abstract
Background:
Literature regarding attitudes towards procreative options in the event of infertility is highly limited.
Objective:
The general aim of the current cross-sectional study is to analyze the relation between basic, personal values (self-enhancement and self-transcendence), and procreative options (living without children, adoption, homologous techniques, and heterologous techniques), while exploring the role of religiosity in moderating this relation.
Methods:
A large sample of 1,891 young Italian adults aged between 18 and 33 was used in the study. The participants were asked to complete a self-report questionnaire. A series of hierarchical regression models were constructed using the SPSS 24.0 software, in order to test the moderation hypotheses.
Results:
Self-enhancement values were positively related to the choice of both homologous and heterologous techniques, whereas self-transcendence values were strong and positive predictors of adoption. Moreover, a significant moderating role of religiosity in shaping the relations between personal values and attitudes towards heterologous techniques emerged: at low levels of self-enhancement values, highly religious participants had a more negative attitude towards heterologous techniques compared to participants with low religiosity. However, self-transcendence values predicted a more positive attitude towards heterologous techniques among participants with low religiosity.
Conclusion:
Findings showed the link between personal values and attitudes towards assisted reproductive techniques and adoption, along with the role of religiosity in shaping this relation; heterologous techniques were the most controversial option according to participants’ perceptions.
1. INTRODUCTION
Becoming a parent has been described as one of the most important transitions in a person’s life, deeply influencing the concept and sense of the self, connecting past and future generations, and helping to build bridges in the community [1]. Research describes couple’s infertility as a shocking experience that has significant negative impacts on the psychological well-being of both individuals; among women, in the form of emotional distress, loss of self-esteem, depression, anxiety, feelings of guilt, frustration, and within the couple in the form of relational and sexual dissatisfaction [2-4].
Individuals and couples who experience infertility have to decide how to face this critical event: whether to live without children, adopt, or search for medical treatments. Indeed, over the past few decades, Assisted Reproductive Technologies (ARTs) have increasingly extended the options for infertile couples to have a biologically related child, questioning the meaning of human conception and parenthood, and replacing other responses to infertility, such as adoption [5]. Research has documented that adoption is viewed as a last alternative to seeking medical treatment [6]. Adoption is often experienced as a “last resort” [7], and most infertile couples decide to adopt only after completely failing extensive infertility treatment procedures [8].
Each option involves complex decisions and potential ethical and moral dilemmas. Without any doubt, the involvement of donors has taken ART on an unexpected turn, generating public debates and ethical concerns [9-11]. This renders the studies on the psychological mechanisms underlying individuals’ procreative behaviors greatly important. The main aim of the current study is to evaluate attitudes towards different procreative options in the event of infertility in a large sample of young Italian adults. In Italy, about 30% of couples are affected by infertility; that is, about 100,000 couples per year experience fertility problems [12]. In this regard, it is relevant to consider the gap between the numbers of children born through ARTs each year (13,973 in Italy, in 2017) [13] and the number of children adopted each year (1,394 international adoptions plus about 1,000 domestic adoptions in Italy, in 2018) [14]. The following procreative options are analyzed here: living without children, adoption, homologous techniques, and heterologous techniques.
1.1. Social Attitudes Towards Procreative Options in the Event of Infertility
Social attitudes help to predict future intentions, plans, and behaviors; they can be resistant to change once formed [15]. As stated by the theory of planned behavior [16], more positive attitudes toward a behavior provide a social context in which that behavior is considered socially acceptable.
Literature regarding attitudes towards procreative options in the event of infertility, especially on non-clinical populations, is highly limited. Globally, studies assessing parenting attitudes in Western countries have evidenced positive attitudes towards adoption and ARTs, and negative attitudes towards a life without children; women are more likely than men to report this preference [17, 18]. Moreover, whereas a general acceptance of ARTs has been found, individuals are more likely to approve homologous techniques than those involving third parties in the process (heterologous techniques or surrogacy) [10, 19-21].
Interesting results were reported in cross-cultural studies. A recent survey involving over 6,000 individuals from 6 European countries (France, Germany, Italy, Spain, Sweden, and the UK) showed that more than half of the respondents (54%) had considered or would consider ARTs treatments – of which, 22% were willing to consider ARTs in case of their partner’s infertility problems and 78% supported gamete donation. Italian respondents, compared to respondents of other countries, reported the lowest level of agreement with accessing In Vitro Fertilization (IVF) for single women and same-sex female couples, and with gamete donation [22]. Indeed, Italy has some specificity to be considered. From a judicial point of view, according to the Law 40 (2004), the access to ART is allowed exclusively to heterosexual, married or cohabitant couples (with no genetically transmittable diseases), to overcome sterility or infertility problems when other therapeutic interventions have proved ineffective. Only in recent years, a series of rulings by the Constitutional Court resulted in the abolishment of the ban on using donor gametes, cryopreservation, and to experiment on human embryos. Surrogacy, however, is not legally recognized. Moreover, from a socio-cultural point of view, Italy appears to adhere to a West-European value model because of the relevance ascribed to individualistic values [23]; however, the Italian culture has some collectivistic aspects as well, being strongly family-oriented [24]. Indeed, Italians are likely to recognize the value of the “psychological” benefits related to the family [25]. Finally, Roman Catholicism is the dominant religion: in 2017, 74.4% of Italian people reported to be Catholics (11.8% not practicing), 22.6% to be atheists, and 3% to be affiliated to other religions [26].
1.2. Religiosity and Attitudes Towards Procreative Options
Religiosity, that is, considering oneself to be a religious person, maybe particularly salient, while taking decisions on how to face infertility [27]. Most religions encourage childbearing and highlight the importance of family ties. Research has shown that higher religiosity is associated with lower acceptance of childlessness [27-29] and higher fertility intentions [30]. Literature has also suggested that persons with higher religiosity tend to be more traditional in choices regarding marriage and family [31, 32] and this may encourage the search for a child.
However, religiosity is also associated with greater ethical and moral concerns about infertility treatments [27, 33]. Most religions discourage or even prohibit the many forms of ART, influencing the type of treatment perceived as acceptable [34-36]. For these reasons, people with strong religious beliefs may choose other options to face infertility. Indeed, religiosity in Western countries was found to be associated with a more positive attitude towards adoption [5, 6, 37-39].
Religiosity is significantly related to values. More specifically, recent literature dealing with religiosity and cross-cultural differences supported the so-called “religiosity as social value hypothesis (RASV)” [40, 41]. Based on this literature, religious cultures (e.g., Pakistan) may embrace religiosity as a social value, leading to religious people feeling pride in fulfilling this value; whereas non-religious cultures (e.g., Belgium) may consider it as a peripheral value. The link between values and religiosity has also been the focus of attention of a relevant meta-analysis carried out on 21 samples from 15 different countries, all adopting Schwartz’s Theory of basic human values [42], as a theoretical framework. According to this study, religiosity is significantly related to peoples’ value priorities. Specifically, in Mediterranean countries, religiosity has been found to be negatively related to conservation and self-direction values, and positively to values of universalism [43].
1.3. Personal Values and Attitudes Towards Procreative Options
Recent research has tried to comprehend which factors predict the different attitudes towards procreative options in the event of infertility. Indeed, at a macro-social-level, attitudes towards childbearing, childlessness, and fertility treatments have changed in Western countries: shifting from more traditional, familistic norms to more individualistic ones, delaying marriage and fertility, as well as considering ARTs to overcome infertility [44-46]. Research has documented that career-focused women are more ethically accepting of donor gamete ART than women who do not place as much importance on the professional success [47]. Other authors [48] suggested that other-oriented people (those assigning more importance to the interests of others) tend to be more motivated to have children and to actually have more children, compared to self-oriented people (those assigning more importance to their own interests).
Despite these relevant and recent findings on the topic, the role of personal values in predicting attitudes towards procreative options in the event of infertility has not been adequately investigated; however, values are likely to influence this variable as they are particularly important for understanding socially relevant concerns [49]. According to the well-known and widely accepted ‘Theory of Basic Human Values’, proposed by Schwartz, values are defined as abstract and trans-situational goals, varying in importance, that guide people’s choices, rendering certain attitudes or behaviors more personally or socially preferable than their alternatives [42, 50].
Schwartz [42] organized values along two bipolar dimensions, thus creating four higher-order value domains. Values that are on the opposite sides of a spectrum are characterized by opposite motivational goals underlying them. The first dimension contrasts conservative values (security, conformity, and tradition), which emphasize order, self-restriction, preservation of the past and the status quo, and resistance to change, with openness to change values (hedonism, stimulation, and self-direction), which instead emphasize the independence of thoughts, actions, and feelings and readiness for change. The second bipolar dimension captures the contrast between self-enhancement values (power and achievement), which emphasize the pursuit of one’s own interests, relative success and dominance over others, and self-transcendence values (universalism and benevolence), which focus on the concerns for the welfare and interests of others, instead. Indeed, while self-enhancement values are characterized by a self-focused goal orientation, namely a concern for the self and for one’s own achievements and goals, self-transcendence values are instead characterized by a social-focused goal orientation, i.e., concern with outcomes for established institutions or for others [51]. Accordingly, the spectrum of literature on this topic has demonstrated how self-transcendence values are related to pro-sociality, helping behavior and caring for others [52-54]. Contrarily, self-enhancement values are related to self-efficacy, self-protection needs, and narcissistic traits, among others [55-57].
1.4. The Present Study
Based on all the above considerations, the general aim of the current study is to analyze the relation between personal values and attitudes towards procreative options in the event of infertility, while exploring the role of religiosity in shaping this link. In pursuing this research aim, we intentionally focused our attention on the value dimension theorized by Schwartz [42], which contrasts self-enhancement and self-transcendence values. Indeed, as already explained in the above section, these value dimensions are prototypical of the contrast between a personal and other-oriented focus [51] and are those more likely to be involved in care and prosocial attitudes [49]. Because of this, we expected this bipolar value dimension to play a role in shaping these kinds of attitudes. This was also done based on previous findings, which emphasized the relevance of personal success and the orientation toward others in influencing attitudes toward procreative options in the event of infertility [47, 48]. Religiosity was also considered as a possible moderator of this relationship because of the different meanings people may assign to values [58]; this is also based on their abstract nature, and to the different attitudes depending on their different level of religiosity. However, because of the scarce literature and due to the exploratory nature of the study, we did not hypothesize the direction of the moderation effect. We also controlled for participants’ socio-demographic variables (sex and age), educational level, and having or not having children.
2. MATERIALS AND METHODS
2.1. Participants and Procedure
The current study derives its data from the database “Rapporto Giovani” (“Youth Report”) launched by the Istituto Toniolo di Studi Superiori with the inclusion of the CARIPLO Foundation and IPSOS LTD as executive partners. Participants were 1891 young Italian adults (Table 1).
The survey was carried out by a mixed methodology: Computer Assisted Telephone Interviewing (CATI: telephone interviews conducted by the interviewer, where answers of the interviewees were inserted by the interviewer directly into the PC); Computer Assisted Personal Interviewing (CAPI: face to face interviews between the interviewer and interviewee, with answers inserted directly by the interviewer into the PC); and, subsequently, going into more depth with Computer Aided Web Interviewing (CAWI: the questionnaire was available online, wherein the interviewees accessed the webpage to answer the questions that appeared on the screen). More technical details are available at this website: https://www.istitutotoniolo.it. Participants were informed about the main objectives of the study, asked to provide informed consent of their participation, and were informed that their participation was free and voluntary. The study was approved by the Scientific Committee of the Family Studies and Research University Centre and followed the APA ethical guidelines for human research (http://www.apa.org/ethics/code/).
2.2. Measures
2.2.1. Socio-Demographic Information
Participants were asked questions about their personal characteristics (sex, age, place of residence, level of education, occupation, and religion) and family life (number of children).
2.2.2. Attitudes toward procreative options in the event of infertility.
To measure the attitude, we developed an ad hoc scenario for this current study. We asked participants to imagine having a friend who is in a heterosexual relationship and is facing difficulties in conceiving; we then asked the extent to which they would advise him/her on each possible solution to face infertility (living without children, adoption, homologous techniques, heterologous techniques). A 5-point Likert-type scale was used to record the responses. For each of the four options, the response scale ranged from 1 = completely disagree to 5 = completely agree. The use of such a scenario allowed us to obtain responses less influenced by ideologies, and collect information on personal attitudes, in an indirect way (thinking about a friend), thus less emotionally connoted.
2.2.3. Personal Values
We used the Italian version of the Portrait Values Questionnaire (PVQ) [59, 60] to measure the importance ascribed to the value dimensions of self-enhancement and self-transcendence. The entire scale is composed of 21 verbal portraits of a person and his/her objectives or aspirations, which implicitly reflect the importance of a value. For example, “It is important for him/her to be rich. He/she wants to have a lot of money and expensive things,” describes a person for whom self-enhancement is important, whereas “He/she thinks it is important that every person in the world be treated equally. He/she believes everyone should have equal opportunities in life” measures self-transcendence, instead. Participants’ values were inferred from their self-reported similarity (from, 1= not like me at all; to, 6 = very much like me) to people described in terms of particular values. We calculated the importance given to the two value dimensions by conducting an average of the items measuring that value. Cronbach's alpha showed good internal consistency: .84 for self-transcendence and .80 for self-enhancement.
2.2.4. Religiosity
To investigate the relevance assigned to religion, we asked participants to answer the question “How important is religion for you?”. Their responses were rated on a scale from 1 = not at all, to 5 = very much.
2.3. Data Analysis
2.3.1. Preliminary Analysis
We described the study variables in terms of means, standard deviations, and range.
2.3.2. Relations between values and attitudes towards procreative options in the event of infertility
After calculating bivariate Pearson correlations among the variables considered, we tested the moderation hypotheses through a series of hierarchical regression models. Specifically, we tested four hierarchical regression models: the four criterion variables were the different attitudes towards procreative options in the event of infertility (living without children, adoption, homologous techniques, heterologous techniques). Based on Baron and Kenny [61], moderation implies that the existing relationship between two variables (in this case, participants’ personal values and their attitudes towards procreative options) changes according to the function of a third variable (in this case, religiosity). We, therefore, labelled this variable “moderator” as it moderates the strength and/or the direction of the relation between the predictors and the criterion.
2.4. Variables
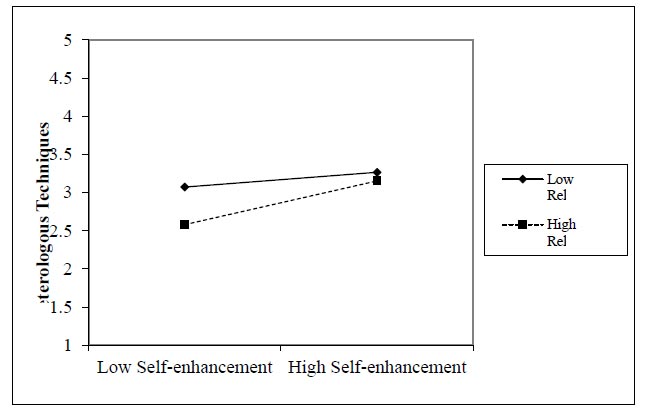
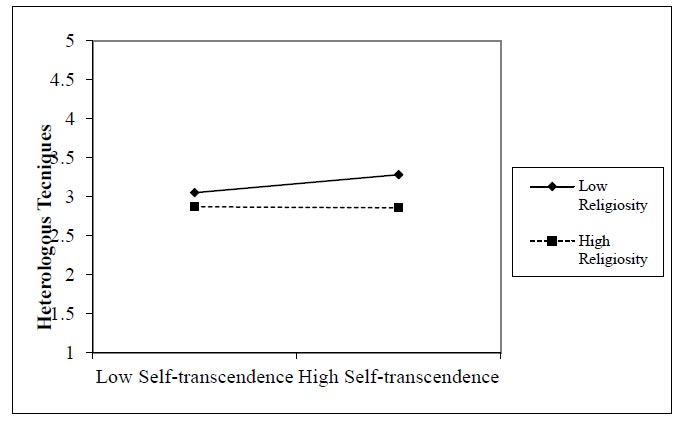
In Step 1, participants’ sex (0=male, 1=female), age, level of education (0=less or equal to 13 years of education, 1=more than 13 years of education), and having or not having children (0=not having children, 1=having children) were entered in the model to control for their effects on the attitudes. In Step 2, the role of self-enhancement, self-transcendence, and religiosity was tested. In Step 3, the interaction terms between self-enhancement and religiosity on the one hand, and self-transcendence and religiosity on the other, were considered. The predictors were grand-mean centered, before carrying out the analysis to reduce multicollinearity [62]. Further interpretation of the significant interactions was achieved through an analysis of the regression slopes [63]. The simple slopes were tested at ±1 SD of religiosity scores (Figs. 1 and 2).
3. RESULTS
Demographics of the participants involved in the study are reported in Table 1. Descriptive statistics of the study variables and their Pearson correlations are reported in Table 2.
Participants showed on average moderate levels of self-enhancement and moderate to high levels of self-transcendence, and medium levels of religiosity. They reported, on average, a moderate to high agreement towards adoption, followed by choice to live without children, homologous techniques, and finally, heterologous techniques.
Self-enhancement and self-transcendence values were positively related to homologous and heterologous techniques. Self-transcendence values were strongly related to adoption, and also positively related to religiosity and the choice to live without children. Contrarily, religiosity was only negatively linked to heterologous techniques, and did not show any other statistically significant correlation with other attitudes towards procreative options in the event of infertility. Finally, Table 3 presents the moderation analyses which test the role of religiosity in shaping the relations between self-enhancement and self-transcendence values on the one hand, and attitudes towards procreative options in the event of infertility, on the other hand.
By analyzing the regression coefficients, we found that older age was related to a positive attitude towards a life without children; specifically, older participants were more prone to suggest this option. Adoption, instead, was more likely to be suggested by women and by participants with a higher level of education.
| Young adults (N = 1891) | ||||
|---|---|---|---|---|
| Variable | N | % | M | SD |
| Sex Female Male |
1220 671 |
64.5 35.5 |
||
| Age | 26.51 | 4.29 | ||
| Place of residence Northwest Italy Northeast Italy Centre South of Italy Abroad |
491 290 316 787 7 |
26 15.3 16.7 41.6 0.4 |
||
| Level of education Middle school High school Undergraduate degree Master degree PhD or second level professional degree |
59 1252 272 223 85 |
3.1 66.2 14.4 11.8 4.5 |
||
| Occupation Students Workers |
559 1332 |
29.6 70.4 |
||
| Having children Yes No |
325 1566 |
17.2 82.8 |
||
| Religiosity No or little importance Moderately relevant Quite or extremely relevant |
863 526 502 |
45.7 27.8 26.5 |
||
| Religious belief Christian Atheistic Private religion Does not express |
1156 399 162 174 |
61.1 21.1 8.6 9.2 |
||
| 1. | 2. | 3. | 4. | 5. | 6. | 7. | |
| 1. Self-enhancement | 1 | .092*** | .046* | .022 | -.011 | .156*** | .189*** |
| 2. Self-transcendence | 1 | .072*** | .098*** | .342*** | .114*** | .066** | |
| 3. Religiosity | 1 | .021 | .004 | .012 | -.146*** | ||
| 4. Living without children | 1 | .217*** | .078** | -.037 | |||
| 5. Adoption | 1 | .217*** | .205*** | ||||
| 6. Homologous techniques | 1 | .393*** | |||||
| 7. Heterologous techniques | 1 | ||||||
| Mean (SD) | 3.04 (.98) | 4.24 (.93) | 2.63 (1.29) | 3.62(1.02) | 3.99 (.92) | 3.26 (.98) | 3.15(.96) |
| Range | 1-6 | 1-6 | 1-5 | 1-5 | 1-5 | 1-5 | 1-5 |
| Predictor | ß | CI | ß | CI | ß | CI | ß | CI |
|---|---|---|---|---|---|---|---|---|
| No children | Adoption | Homologous techniques | Heterologous techniques | |||||
| Step 1 | R2=.003 | R2=.012 | R2=.001 | R2=.002 | ||||
| Sex | -.002 | [-.101, .093] | .084*** | [.075, .249] | -.007 | [-.107, .080] | .042 | [-.006; .177] |
| Age | .053* | [.001, .024] | -.027 | [-.016, .004] | .002 | [-.010, .011] | -.012 | [-.013; .008] |
| Education | -.006 | [-.114, .088] | .054* | [.018, .198] | .031 | [-.031, .163] | -.016 | [-.129; .061] |
| Children | .052 | [-.152, .107] | -.018 | [-.159, .073] | .024 | [-.061, .188] | -.006 | [-.138; .008] |
| Step 2 | R2=.013 | R2=.122 | R2=.035 | R2=.068 | ||||
| Self-enhancement | .017 | [-.030, .065] | -.040 | [-.078, .003] | .147*** | [.103, .194] | .200*** | [.154; .241] |
| Self-transcendence | .099*** | [.059, .159] | .339*** | [.292, .378] | .101*** | [.059, .154] | .056* | [.012; .104] |
| Religiosity | .011 | [-.028, .044] | -.018 | [-.043, .018] | -.005 | [-.038, .030] | -.162** | [-.154; -.088] |
| Step 3 | R2=.0.15 | R2=.124 | R2=.035 | R2=.081 | ||||
| Self-en.* Rel. | -.042 | [-.066, .003] | .022 | [-.014, .045] | .005 | [-.030, .036] | .104*** | [.043; .106] |
| Self-tr.* Rel. | .021 | [-.021, .056] | .025 | [-.014, .051] | .001 | [-.035, .037] | -.064** | [-.086; -.016] |
When considering values, it is relevant to note that self-enhancement was a positive predictor of a positive attitude towards both homologous and heterologous techniques. Self-transcendence was instead a positive predictor of all options presented to cope with infertility, although the regression coefficient was higher when considering the possibility of adoption. However, only religiosity was found to significantly and negatively influence heterologous techniques; religiosity moderated the relations between participants’ personal values and their attitudes towards heterologous techniques, also when controlling for sex, age, level of education, and having or not having children. In particular, at low levels of self-enhancement values, highly religious participants had a more negative attitude towards heterologous techniques compared to those with low religiosity, whereas at high levels of self-enhancement, no differences emerged. In particular, the positive relation between self-enhancement values and a favorable attitude towards heterologous insemination was stronger for highly religious people. On the contrary, the positive relation between self-transcendence values and a favorable attitude towards heterologous insemination was stronger for people with low religiosity. Nonetheless, self-transcendence values were found to predict a more positive attitude towards heterologous techniques at low levels of religiosity.
4. DISCUSSION
The current study was aimed at analyzing the relation between personal values and attitudes towards different procreative options in the event of infertility, while exploring the role of religiosity in forming this link. Overall, our results showed that in the event of infertility, participants were more likely to advice to adopt a child, highlighting a positive attitude toward this form of parenthood. Contrary to studies involving other countries [17, 18], for Italian young adults, ARTs, especially heterologous techniques, were less recommended, even in comparison to living without children. With regard to their personal values, participants assigned greater importance to self-transcendence values compared to self-enhancement values; this is in alignment with previous studies, which investigated the value priorities of young Italian adults [e.g., 64]. Participants also exhibited an overall medium level of religiosity.
From the correlation analysis between both self-enhancement and self-transcendence values, the different attitudes towards procreative options in the event of infertility, and from the regression models, two of the most relevant patterns emerged. First, the option to adopt a child when coping with infertility is significantly, positively, and strongly associated with self-transcendence. This positive relationship may be due to the fact that self-transcendence values are by definition other-oriented and altruist goals, associated with the dimension of social justice [51], while adoption can assume the notion of becoming generative at the social level, by taking care of children “born by others” [1, 65, 66]. Second, the more young adults give importance to self-oriented values, the more they show a positive attitude towards ARTs, both homologous and heterologous: having a child may be perceived as a personal goal and success, a form of self-realization which can also be pursued, with these techniques. This positive relation – albeit smaller in size – was, however, also found between these same two attitudes (i.e., homologous and heterologous techniques) and self-transcendence values, which may encourage interest in and search for new lives and relations. We may also speculate that to some universalism, a dimension of self-transcendence (an item example for universalism values is: “He/she thinks it is important that every person in the world be treated equally. He/she believes everyone should have equal opportunities in life”), could be interpreted as the “right for a child,” thus associating with positive attitudes toward ARTs in the event of infertility to pursue this goal. Finally, correlation analysis and regression models also showed that religiosity was negatively linked to heterologous techniques; specifically, young adults, who place higher importance on religiosity in their lives, are less prone to show a positive attitude towards this method to cope with infertility. Religiosity, in particular for Catholic young adults that are the most represented in our sample, is associated with greater ethical and moral concerns about medical techniques that include external third parties who aid the couple to conceive [27], confirming, again, that it is perceived as the most controversial option by Italian respondents.
Moreover, our study also focused on the role of religiosity in shaping the existing link between personal values and the different attitudes towards procreative options in the event of infertility. The results highlighted that religiosity has a non-significant moderating role in the relation between personal values and all the procreative options, with the only exception of heterologous techniques confirming that it is the most controversial procreative option in the Italian context. In this case, the moderating role of religiosity was found also when controlling for sex, age, level of education, and having or not having children. Specifically, at low levels of self-enhancement values, highly religious participants had a more negative attitude towards heterologous techniques compared to those with low religiosity. This result made us speculate that when religiosity is less associated to self-oriented values, it may negatively influence one’s attitude towards heterologous techniques; when religiosity is instead associated with a strong focus towards the self, it may assume the meaning of a “personal” religion, untied from the more traditional concept of religious faith, thus associating with a more positive attitude towards heterologous techniques. The other relevant result highlighted instead of how self-transcendence values may promote a positive attitude towards heterologous techniques to a greater extent at low levels of religiosity. In this case, we may speculate that for an individual who considers religion relevant in his/her life, self-transcendence values are more proxy to the traditional Western vision of morality about how people should relate to each other, to preserve the wellbeing of others [67]. Thus, heterologous techniques are probably perceived as less accepted behaviors. For an individual who instead does not consider religion relevant in his/her life, self-transcendence values could mean equal rights for everyone, thus positively associating with attitudes towards heterologous techniques. All in all, according to our expectations as well as previous literature [58], religiosity can affect the meaning as well as the relation between values and attitudes towards procreative options in the event of infertility.
CONCLUSION
To our knowledge, our study is among the firsts of the kind to focus on the role of personal values influencing the possible attitudes towards procreative options in the event of infertility. However, some limitations should also be considered. First, we exclusively used self-report measures. Second, though personal values and religiosity are useful in explaining some attitudes towards procreative options in the event of infertility (adoption and heterologous techniques), other factors should be considered when explaining other options (living without children and homologous techniques). The low portion of explained variance highlighted the complexity of the explored relation. Therefore, personal values and religiosity seem to be useful in explaining some attitudes towards procreative options in the event of infertility (adoption and heterologous insemination), but other factors should be considered when aiming at explaining other options (child-free living and homologous insemination). Intervening variables in the relation between attitudes and social behaviors should be considered when interpreting our results and some potential confounding variables (e.g., an individual’s psychological well-being and sentimental status) should be included, in order to obtain a complete portrait of this relation, in the future. Finally, the study is cross-sectional, which limits the opportunity of causal inferences. Longitudinal studies are required to confirm the intensity and direction of these relation. Despite the aforementioned limitations, our results may be informative for professionals working in the field of infertility and adoption. Research on factors having an impact on attitudes towards procreative options in the event of infertility, could lead to the development of more effective counselling strategies for fertility patients who, in turn, are also prospective adoptive parents. Our data suggest the critical role of personal values as well as religiosity in shaping an individual’s attitude, which should be considered while providing interventions.
ETHICS APPROVAL AND CONSENT FOR PUBLICATION
The study protocol was not reviewed by the ethics committee since it was not required at the time of data collection, according to the local and national guidelines. However, it was approved by the Scientific Committee of the Family Studies and Research University Centre and it allowed the standard ethical guidelines of the Italian Association of Psychology (AIP) and the standard ethical guidelines of the American Psychological Association (APA).
HUMAN AND ANIMAL RIGHTS
Not applicable
CONSENT FOR PUBLICATION
All the participants included in the present study gave their informant consent.
AVAILABILITY OF DATA AND MATERIALS
The datasets for this manuscript are not publicly available because of local, legal and privacy restrictions (Italian Data Protection Code – Legislative Decree No. 196/2003). However, the raw data supporting the conclusions of this manuscript can be made available by the first author upon reasonable request.
FUNDING
This work was financially supported by the Istituto Toniolo di Studi Superiori.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The researchers would like to express their gratitude to all the participants that agreed to be involved in this research project, sharing with us their experiences.

