All published articles of this journal are available on ScienceDirect.

The Role of Resilience towards the Correlation between Adverse Childhood Experiences and Post-Traumatic Growth
Authors Info & Affiliations
Abstract
Background:
Positive changes may occur in someone after experiencing a traumatic childhood. Previous research found that Adverse Childhood Experiences (ACEs) could not be the only factor that becomes the cause for an individual’s Post-Traumatic Growth (PTG); thus, research that describes the role of a mediator in both variables is needed. Since studies investigating ACEs among Indonesia participants are still lacking, this would be considered as initial research on the relations of ACEs and PTG.
Objective:
This research was aimed to investigate how resilience becomes a mediator between children’s traumatic experiences of ACEs and PTG.
Methods:
This research used a quantitative correlational method to investigate the relation between the three examined variables: Adverse Childhood Experience (ACEs), Resilience, and Post-traumatic Growth (PTG). A total of 349 participants were participated in this research, with the age range from 12 to 65 years old, predominantly female (N = 271;77,7%). Three research instruments were used in this study, such as the Adverse Childhood Experiences scale, Connor Davidson Resilience Scale, and Post Traumatic Growth Inventory (PTGI).
Results:
The results showed a significant correlation between Adverse Childhood Experiences, Resilience, and Post-Traumatic Growth. A Structural Equation Modelling (SEM) analysis revealed a nonsignificant impact from ACEs to PTG. Resilience is proven to play the role of a mediator in the relation between ACEs and PTG, which was shown using the submitted model plot that revealed a higher total effect after resilience was placed as the intervening variable (standardized total coefficient = –.192). Details on mediating effects of each resilience factor were presented and explained further, along with the discussion on Indonesia's cultural background.
Conclusion:
This article revealed the connection between the ACE that the individual experienced in the past with resilience and PTG. Indonesian-related culture and characteristics were also explained.
1. INTRODUCTION
Children who were abused during childhood often have to live a traumatic experience because most of the time, the abuser is from their own family. The data obtained from the Ministry of Empowerment of Women and Children Protection of the Republic of Indonesia in 2019 showed that 33% of the children abused were within 0-12 years old. The abuse was in the form of physical (28%), psychological (23%), and abandonment (7%) abuse. A traumatic incident experienced by children is called Adverse Childhood Experience [1, 2]. This ACEs traumatic experience may severely affect mental health and have a negative impact on social and psychological life, in addition to physical health, that makes people antisocial. Individuals who experienced the trauma would experience a lot of changes in their lives. However, not all traumatic experiences affect someone’s life badly because some people who experienced trauma might develop a better life than before. Positive changes may occur to somebody after experiencing a traumatic childhood.
An individual’s positive change after a post-traumatic event is termed Post-Traumatic Growth (PTG). PTG is a positive impact for someone who decides to struggle positively with their trauma. Examples of positive PTG include seeking a meaningful life, making positive changes like getting up from rock bottom experiences, and making psychological improvements about their condition [3]. PTG is a psychological change that happens cognitively and emotionally to individuals as a result of their traumatic events in the past, which may be related to themselves, other parties, and the future [4, 5]. An individual’s positive change results from a process of facing lots of changes, struggles, and other challenges, which upgrades someone’s higher cognitive functional adaptation [6]. Calhoun and Tedeschi [7] divide PTG into five domains: a. Personal Strength is when someone would report positive changes and describe himself as a better person. Being stronger, more creative, more confident, and are open to the different changes that may happen to be a better individual; b. Relating to others is when someone would show development when having a better relationship with their family, friends, or people who experience the same traumatic event; c. Encompasses Appreciation for life is when someone reports having a clear vision about what is important in life and could rearrange his priorities in life through many aspects, such as the increase of existential consciousness; d. New Possibilities is when someone shows a desire to change his life’s direction by learning some new knowledge and skills after enduring a traumatic experience; e. Spiritual Change is when someone shows how to actively participate and have faith in higher beings.
Some research works show a negative correlation between pressure and PTG, which means if the individual develops a higher PTG experience, his/her perception toward past difficulties will likely drop and will be able to overcome cognitive problems. According to that research, it is important to investigate the factors that will help someone who experiences ACEs to develop PTG in the next development. To achieve PTG, it is affected by some general factors. One of those factors is a psychological factor [8]. Traumatic experiences imply some negative circumstances that may cause suffering, vulnerability, uncertainty, and lack of one’s life control. Putting them all together, someone may have a perception of what becomes the benefits of being a survivor from trauma [7, 9].
The PTG terminology, introduced firstly by Tedeschi and Calhoun [9], is related to the positive change that involves the perception of the self by others. It occurs in conjunction with the life appreciation that arises as a consequence of the attempt to handle the traumatic life experienced by the PTG so that a balanced life can be achieved from the coping mechanism. This phenomenon shows that the effects of the trauma undergo a transformation, thereby increasing compared to the initial stage of the trauma. Tedeschi and Calhoun [7] referred to this phenomenon to understand how the PTG was formed as a result of the cognitive involvement of a deeper understanding of what happened to the self and the world. The mechanism of PTG is associated with cognitive reconstruction and the events that determine someone’s future.
One’s endurance in facing an unpleasant event can affect how far someone reaches PTG. The quality possessed by someone when facing life difficulties can be seen from how more capable he would be in handling a difficult situation and being resilient [10]. This is supported by a study conducted by Mahdi et al. [11], who concluded that two dimensions of resilience, adaptive capacity, and positive acceptance, had a significant impact on PTG after undergoing a traumatic event. The meaning of psychological resilience by scholars, in general, is the existence of a positive adaptation in facing difficulties [10]. Resilience is then usually explored in various contexts, which have different levels from mild hassles (e.g., work stress) to severe trauma (e.g., mourning, life-threatening events). Many factors contribute to resilience, including personal factors, such as spirituality, optimism, positive emotions, cognitive flexibility, active coping, and acceptance, as well as biological and environmental factors (e.g., relationships with family and peers, a sense of social belonging), which can be considered as a source of resilience [12, 13].
Resilience is related to PTG since it is depicted as the recovering ability to return back to the time when the difficulties happened with only a minimal reaction after that event [14]. It is a fact that resilient individuals actually have above-average skills in communication, cognitive, and problem-solving abilities. In addition, it is also related to having a high self-confidence in the future, the ability to manage their attitudes, self-appreciation towards life, good relation to other people, inner strength, new possibilities, and spiritual development, so that PTG could grow as a result of the trauma or crisis experience [9].
Liu et al. [15], in their studies, conveyed that a harmful childhood with ACE is known as having risks of several social, economic, and health issues in their lives. Meanwhile, resilience is known as the protective factor for children to make an upswing from their bad childhood experience. Research from O’Malley et al. [16] showed that ACE is related to the resilience undergone during adolescence and early adulthood. The resilience was formed from aspects, such as the ability to adapt, tolerance for negative effects and reinforcement from stress, perception of control, and persistence in its role as a mediator for ACE, which may increase the experience of post-traumatic growth that is manifested as a personal strength and an appreciation of life [9, 17]. As illustrated, resilience with the before-mentioned dimensions will increase PTG due to the benefit of obtaining a positive change after experiencing a difficult childhood ACE or other challenges [17].
1.1. Research Objectives
This study aimed to figure out the role of resilience as a mediator in the relation between Adverse Childhood Experiences (ACEs) and Post Traumatic Growth (PTG). Two hypotheses were proposed in this research: the traumatic event experienced in childhood has a correlation with post-traumatic growth, and resilience has a positive impact on the post-traumatic growth the individual experienced which was the result of ACEs.
2. METHODS
2.1. Research Procedure
A quantitative correlational method was used in this research to investigate the relation between the three examined variables: Adverse Childhood Experience (ACE), Resilience, and Post-traumatic Growth (PTG). The data were taken online using Google Forms filled by the participants who fit with the criteria for this research. Prior to the research, all participants were given a chance to give their consent in an Informed Consent form. The participants who agreed were then included in this research. The research discussed here had been approved by the Ethics Committee of the Faculty of Psychology, Soegijapranata Catholic University (Approval Number: 005/B.7.5/FP.KEP/IV/2021).
2.2. Research Participants
The population for this research was 12-year-old individuals who experienced unpleasant incidents or traumatic experiences in childhood and were living in Indonesia. In this research, the researchers used convenience sampling to gather the data obtained by filling an online form conducted using Google forms published via Facebook, Instagram, Twitter, WhatsApp, and other Social Networking Sites (SNS). Data were collected for approximately three months, from December 2020 to February 2021. A total of 349 respondents provided the collective profile described, participants from adolescents up to elderly and mostly female (77.7%), and the majority graduated from high school (60.5%%).
2.3. Research Instruments
Three research instruments were used in this research:
Adverse Childhood Experiences Inventory: The instrument was used to measure 10 kinds of childhood trauma. The items on the ACE checklist were divided into two parts: the first part comprised five items that contained direct trauma to the participants, such as violence in the form of physical abuse, verbal abuse, sexual harassment, physical abandonment, and emotional abandonment. The second part also consisted of five other items, which contained things that were related to other families. The ACE applied in the research was developed by Felitti et al. [18]. This research participant comprised alcoholic parents, an abused mother, imprisoned family members, family members with mental illness, and divorced parents.
Connor Davidson Resilience Scale: Resilience as the mediator variable in this research was measured using the resilience scale, which was interpreted from Connor and Davidson’s Resilience Scale [10]. This scale, like Likert Scale, consisted of 5 scores starting from 0 ‘not right at all’, to 4 ‘almost always right.’ This scale comprised of 25 items, which was divided into 5 aspects to depict the resilience construct based on the previous research by Connor and Davidson, including 1) personal competency, high standard, and persistence; 2) belief in instinct, negative effect tolerance, and empowerment from the effect of stress; 3) positive acceptance towards changes and a friendly relation; 4) control; and 5) spiritual impact.
Post Traumatic Growth Inventory: PTGI translated into Bahasa Indonesia was used to measure the level of Post-Traumatic Growth [19, 20]. The PTGI that was used to calculate the dependent variables in this research comprised of 21 items that had a scale of 6 scores in each item starting from 0 ‘I did not feel any changes after my crisis,’ to 5 ‘I felt big changes after my crisis.’ A series of aspects measured in this scale to examine the PTG experienced by the participants were: 1) personal strength; 2) life appreciation; 3) relationship with other people; 4) new possibilities; 5) and spiritual changes.
2.4. Data Analysis Procedure
The acquired data in this research were processed using an IBM SPSS for Statistics 26 and IBM SPSS AMOS 23. Three main variables will be analysed in this research, ACEs as the independent variable, PTG as the dependent variable, and resilience, which is expected to play the mediating role in the relationship between independent and dependent variables. CD-RISC and PTGI measuring instruments that had been translated were used to measure constructed validity using Confirmatory Factor Analysis. The scattered items and aspects of the data obtained were checked with previous findings. Besides, demographical data will also be included in this article, which is presented in the results section as well. A set of Pearson’s correlation tests (one-tailed) were conducted to explore associations between variables and their factors. To test the main hypotheses, the researchers used Structural Equation Modelling (SEM) with the help of IBM SPSS AMOS 23. It was expected that resilience takes the mediating role in the relations between ACEs and PTG; whether the mediating effect was partial or complete mediation also be investigated statistically. In addition, path analysis was performed to investigate the mediating role of each resilience factor in this study framework. Throughout the report, we used the significance threshold (α) of .05.
3. RESULTS
In this research, there were 349 participants who were within the age gap of 12 – 18 years old until 65 years old. As shown in Table 1, most were female (N=271; 77,7%). The educational background of the respondents was varied from elementary school to post-graduate. Most of them were high-school graduates, i.e., 60.5% (N = 211). Most of the participants were also single (N = 296; 84.8%). A total of 59 participants were married (14.9%), and the rest of the participants were divorced. The status and occupation of the participants were mostly students (from high school to university level). Data for this demography were noted as 60.5% (N=211).
| Variable | Category | Percentage |
|---|---|---|
| Sex | Male | 22.3 |
| Female | 77.7 | |
| Age | 12-18 | 14.6 |
| 18 - 29 | 71.3 | |
| 30 - 39 | 7.2 | |
| 40 - 49 | 2.9 | |
| 50 – 60 | 1.1 | |
| > 60 | 2.9 | |
| Education Background | Elementary | 2.6 |
| Junior High | 7.7 | |
| Senior High | 60.5 | |
| Undergraduate | 23.5 | |
| Graduate | 4.6 | |
| Postgraduate | 1.1 | |
| Marital Status | Single | 84.8 |
| Married | 14.9 | |
| Divorced | .3 |
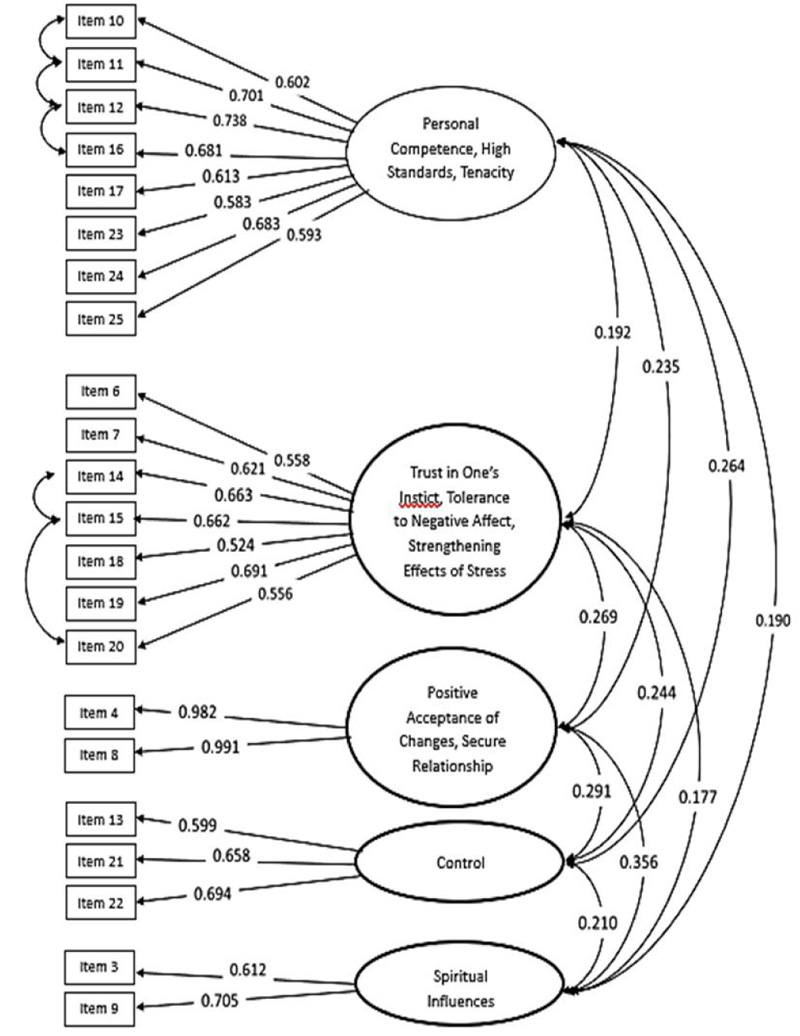
As for PTGI, the CFA result showed that the adaptation of the PTGI scale had a good Model Fit (GFI = .904, CFI = .913, RMSEA = .063) with standardized items’ loading factors ranging from 0.584 to 0.785, as seen in Fig. (2). Furthermore, the Alpha Cronbach Reliability test’s results showed that the adaptation of the CD-RISC scale and PTGI have good reliability with CD-RISC’s alpha score, which was .927 and .931, respectively.

To obtain the mean and SD for each variable, bivariate correlation tests were executed to test the correlation between each variable in the research. Based on the data findings, a significant negative correlation between ACE and resilience was found (r = - .202). A similar correlation but weaker result was shown amongst the ACE and PTG (r = - .187). In addition, it is shown in Table 2 that all of the resilience factors are significantly associated with ACEs, Post-Traumatic Growth, and all of their aspects. Meanwhile, not all aspects of Post-Traumatic Growth showed a statistically significant correlation with ACEs. This means that even though ACE was related to PTG to some extent, a stronger correlation was shown between ACE and resilience. That makes this finding support the offered model. Concerning the relationship between resilience and PTG, the correlation test result showed a significantly positive relationship.
| No. | Variable | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. | Total PTG | 69.96 | 13.79 | |||||||||||||
| 2. | Relating to Others | 24.88 | 5.36 | |||||||||||||
| 3. | New Possibilities | 17.26 | 3.82 | |||||||||||||
| 4. | Personal Strength | 13.96 | 3.14 | |||||||||||||
| 5. | Spiritual Changes | 6.72 | 1.99 | |||||||||||||
| 6. | Appreciation to Life | 7.14 | 1.75 | |||||||||||||
| 7. | Total Resilience | 61.64 | 11.96 | .566* | .463** | .522** | .519** | .417** | .498** | |||||||
| 8. | Factor 1: Personal Competence, High Standard, and Tenacity | 23.11 | 4.74 | .569** | .469** | .544** | .515** | .393** | .492** | |||||||
| 9. | Factor 2: Trust in One’s Instinct, Tolerance to Negative Effect, Strengthening Effects of Stress | 17.90 | 4.25 | .464** | .357** | .449** | .441* | .340** | .407** | |||||||
| 10. | Factor 3: Positive Acceptance of Changes and Secure Relationship | 5.58 | 1.87 | .348** | .300** | .261** | .341** | .292** | .314** | |||||||
| 11. | Factor 4: Control | 8.61 | 1.94 | .464** | .397** | .420** | .422** | .316** | .405** | |||||||
| 12. | Factor 5: Spiritual Influences | 6.42 | 1.37 | .399** | .338** | .333** | .317** | .383** | .377* | |||||||
| 13. | Total ACE | 1.46 | .879 | -.187** | -.188** | -.166** | -.155** | -.085 | -.159** | -.202* | -.138* | -.179** | -.162** | -.169** | -.269** | -.187** |
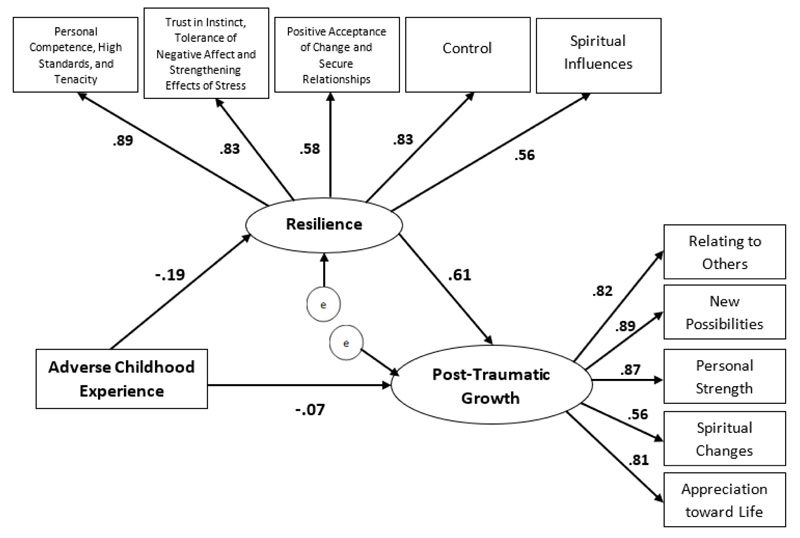
To test the hypotheses, the researcher used Structural Equation based analysis with all 349 participants using AMOS software. Based on the data analysis, the offered hypothetical model in this research indicated a good fit with the data collected (Fig. 3). The CFI score was .997, TLI was .96, and RMSEA was .065. ACE was shown to have a significantly negative relationship towards resilience (standardized coefficient = -.19) and a non-significantly negative relationship towards PTG (standardized coefficient = .61). This research proposed a hypothesis that the correlation between ACE and PTG has an indirect effect relationship with mediated resilience. Fortunately, this research supported the hypothesis because it revealed a significant indirect correlation between ACE and PTG through resilience (standardized indirect coefficient = -.12). Moreover, the proposed model plot revealed by the analysis result showed a higher total effect in comparison to the direct effect (standardized total coefficient = -.192).
In order to confirm the mediating effects of each factor of resilience, in this research, we used Hayes’ (2013) PROCESS software based on the proposed mediation model. PROCESS uses a path analytical framework and bootstrapping to provide powerful estimates of direct and indirect effects in mediation models. We altered the initial mediating variable, resilience, into its factors. The total effect of collectivism on environmental quality was significant, β = -.19, SE = .828, p = .000, 95% CI (-4.56, -1.30), as seen in Fig. (4). The result, as shown in Fig. (5), thus, implies that Factor 1 (Personal Competence, High Standard, Tenacity) has no mediating effects on the relation between ACEs and PTG. The direct effect controlling for Factor 1 of resilience was also significant but smaller in size, β = -.11, SE = .69, p = .013, 95% CI (-3.09, -.36), and the associated indirect effect was nonsignificant, β = -.08, SE = .041, 95% CI (-.16, .002).

Note: * = sig <.05 ; ** = sig <.01, βc = β coefficient between dependent and independent variable (total effect).
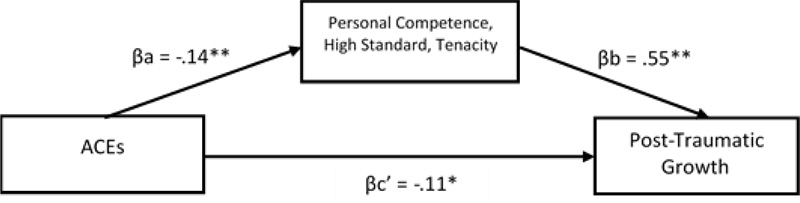
Note: * = sig <.05 ; ** = sig <.01 ; βc’ = β coefficient between dependent and independent variable (direct effect) ; βa = β coefficient between independent variable and mediator ; βb = β coefficient between mediator and dependent variable.
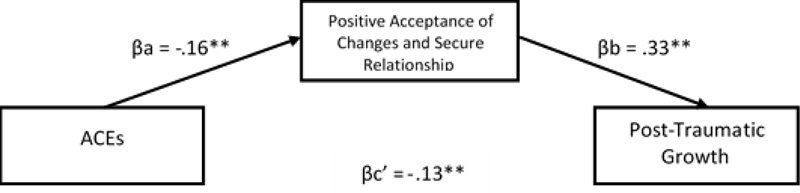
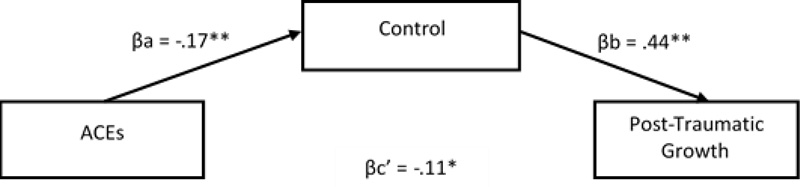
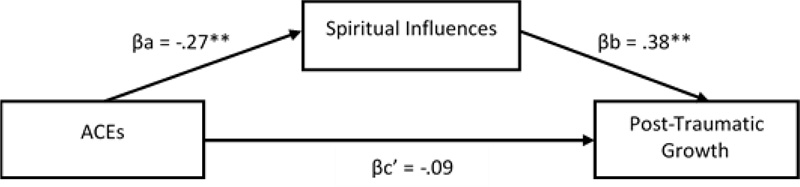
Apart from Factor 1 that showed no mediating effect, the rest of the resilience’s factors showed mediating effects. In detail, Factor 2, as shown in Fig. (6) (Trust in One’s Instinct, Tolerance to Negative Affect, Strengthening Effects of Stress), 3, as in Fig. (7), (Positive Acceptance of Changes and Secure Relationship), and 4, as shown in Fig. (8), (Control) showed partial mediating effects while Factor 5 (Spiritual Changes) showed full mediating effect, as shown in Fig. (9). The direct effect control for Factor 2 of resilience was significant but smaller in size, β = -.11, SE = .75, p = .027, 95% CI (-3.16, -.19), and the associated indirect effect was also significant, β = -.08, SE = .036, 95% CI (-.15, -.01). The result of direct effect control for Factor 3 of resilience was also shown significant but smaller in size, β = -.13, SE = .79, p = .008, 95% CI (-3.66, -.54), and the associated indirect effect was also significant, β = -.05, SE = .023, 95% CI (-.10, -.01). Showing a similar pattern, the direct effect control for Factor 4 of the resilience was significant but smaller in size, β = -.11, SE = .75, p = .020, 95% CI (-3.24, -.27), and the associated indirect effect was also significant, β = -.08, SE = .027, 95% CI (-.13, -.03). There is, however, a slightly different result in the direct effect control for Factor 5 of resilience, which was nonsignificant, β = -.09, SE = .80, p = .093, 95% CI (-2.92, .22), and the associated indirect effect that was significant, β = -.10, SE = .048, 95% CI (-.19, -.03).The summary of the beta effects of each factor is presented in Table 3 below.
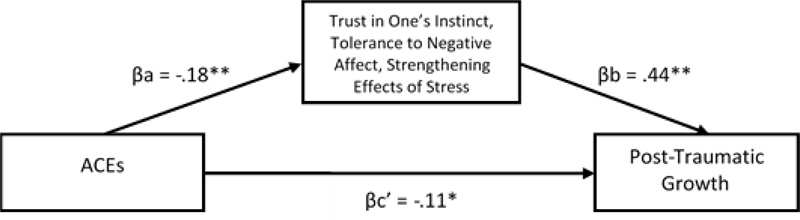
Note: * = sig <.05 ; ** = sig <.01 ; βc’ = β coefficient between dependent and independent variable (direct effect) ; βa = β coefficient between independent variable and mediator ; βb = β coefficient between mediator and dependent variable.
Note: * = sig <.05 ; ** = sig <.01 ; βc’ = β coefficient between dependent and independent variable (direct effect) ; βa = β coefficient between independent variable and mediator ; βb = β coefficient between mediator and dependent variable.
Note: * = sig <.05 ; ** = sig <.01 ; βc’ = β coefficient between dependent and independent variable (direct effect) ; βa = β coefficient between independent variable and mediator ; βb = β coefficient between mediator and dependent variable.
Note: * = sig <.05 ; ** = sig <.01 ; βc’ = β coefficient between dependent and independent variable (direct effect) ; βa = β coefficient between independent variable and mediator ; βb = β coefficient between mediator and dependent variable.
| No. | Mediating Factor | Direct Effect (95% CI) | Indirect Effect (95%CI) |
|---|---|---|---|
| 1 | Personal Competence, High Standard, Tenacity | βc' = -.11 (-3.09, -.36) | βc = -.08(-.16, .002) |
| 2 | Trust in One’s Instinct, Tolerance to Negative Effect, Strengthening Effects of Stress | βc' = -.11(-3.16, -.19) | βc = -.08 (-.15, -.01). |
| 3 | Positive Acceptance of Changes and Secure Relationship | βc' = -.13 (-3.66, -.54) | βc = -.05 (-.10, -.01) |
| 4 | Control | βc' = -.11 (-3.24, -.27) | βc = -.08 (-.13, -.03) |
| 5 | Spiritual Changes | βc' = -.09 (-2.92, .22) | βc = -.10 (-.19, -.03) |
4. DISCUSSION
This research was conducted to reveal the correlation between ACEs, resilience, and PTG. The proposed hypothesis was that ACEs were related to the PTG experienced by the individuals. The correlation test’s results showed that ACEs, indeed, had a significant correlation with PTG. This was in line with the research conducted by Schubert et al. [21], who believed that individuals experiencing hardships in their family had a correlation with PTG achievement. Bad experiences in childhood have positively predicted PTG in children [22]. Another study showed a similar result, like the study conducted by Shand et al. [23]. They found a similar result in their study, whereby individuals who experienced bad times in childhood did not always have a negative impact when they grew up. Many children could have had a stronger personality and could have been empowered by resilience. That study result supported this recent research, where ACEs were experienced by individuals in the past and had a significant correlation with the individuals’ level of resilience. All of the previous research reviewed revealed a connection amongst variables, which was explained by the details that ACEs had a significant correlation with resilience and PTG. The stronger correlation between resilience and PTG indicated that the relation ACEs had with PTG was mediated by resilience, like how it was hypothesized from other studies.
Further analysis using SEM showed that ACEs were insignificantly impacted directly by resilience. This result supported some arguments proposed by some related studies, whereby ACEs as experiences could not be the only predictor of psychological problems (including PTG as a positive growth) without going through other processes [24, 25]. In other words, to reach a certain level of PTG, individuals need to cope with post-trauma stress through a cognitive learning process aided by resilience as one of the internal models [7], [21, 23]. The findings and theoretical background have helped the offered model in this research, where resilience works as the mediator that increases the significant indirect impact of ACEs towards PTG.
Theoretically, the increased PTG was related to the dimensions of resilience, which later will increase PTG or benefit finding along with psychological growth to a positive side because of the experience obtained from ACEs or other hurdles to achieve a higher functional level [17]. Another argument conveyed by Malhotra and Chebiyyam [26], who did a study on PTG as a result of bad events in life, could be concluded that the growth was a result from the struggle to prevent the traumatic experience and how the individuals find a meaningful life, which sprang not from the bad experience itself. The process to prevent that crisis or the traumatic event had been predicted by the resilience that the individuals owned, as concluded by Tranteret al. [27]. This explanation, then, may describe how resilience played the role of a mediator between the ACEs and PTG that the individuals were experiencing.
Furthermore, we also found that some aspects of PTG were significantly associated with ACEs, although it was then revealed that resilience plays a partial mediation role in the relationship of those two variables. ACEs as traumatic events occur during childhood, and they are more likely to be part of a person's identity, which serves as a developmental basis for understanding, thinking, and reacting to living circumstances [20]. However, since the self is complex and constructed, individuals have a choice in the formation of their identity. Thus, adults are not destined to have the self-concept of their childhood [28]. When a person experiences personal development by facing the difficulties of his life, that person will have a broader perspective on the development of personal resources [7, 29].
In a more detailed analysis, the results showed that personal competence, high standard, and tenacity factors did not provide a mediating effect on the relationship between ACEs and PTG levels. Qualitative research among Indonesian people showed that strong spiritual factors and social support affect PTG more than confidence in self-strength [30]. This is due to the more collective type of Indonesian society, which does not give too much encouragement for the individual self-confidence to grow after traumatic events. In addition, another factor of resilience, which is spiritual influence, actually provides the strongest mediation effect on the relationship between ACEs and PTG in the Indonesian community. These results support previous research on PTG in Indonesian and Asian communities by showing that spirituality and religious activity significantly predict PTG levels in survivors of natural disasters [31, 32]. Actually, not only in the face of traumatic events, Subandi et al. [32] explained that in facing difficulties, in general, Indonesian people in Java, who are Muslims, adopt more religious and/ or spiritual coping techniques, such as dhikr (doing remembrance rituals to God), salat (doing daily prayer), sabar (be patient), nrimo (be warmly accepting things), tawakkal (ready to surrender), and bersyukur (give gratitude).
This study provides supporting evidence and new knowledge regarding the relationship of ACEs as traumatic events from the past (outside the context of natural disasters in previous studies) with the PTG level of the Indonesian society. It is strongly mediated by spirituality, which is a factor of resilience as a complete mediator. In more detail, Akbar [33] explained how spirituality is believed to be sacred by the people of Indonesia and can encourage positive growth by providing a sense of security and deeper meaning to the painful events experienced.
4.1. Limitations
Even though the research could reveal the result that depicted the role of resilience in ACEs and PTG correlation clearly, this research had some limitations that could be overcome further in the next research. Firstly, participants of the current study included a wide age range and seemed not evenly distributed (mostly early adulthood and incorporated the small data of elder participants). However, despite a wide age range, data gathered are all, in fact, statistically normally distributed, so the authors decided to include the whole dataset in order to capture growth experienced by participants from different generations. Second, this research aimed to investigate the role of resilience as a mediator, while other researchers believed that there were lots of different factors that may protect and support in time of post-trauma crisis [34-36]. Therefore, future research could investigate other factors that may be the mediators between PTG and ACEs, which would provide a bigger picture of the phenomenon. Data of this research only represented what happened in Indonesia with Indonesian participants. Thus, there is still a need to do further research to involve a wider population considering the cultural and social aspects through theoretical reviews and other similar research.
CONCLUSION
This article revealed an association between the ACE that the individual experienced in the past with resilience and PTG. ACE was found to have a significant correlation with the level of PTG someone was experiencing, but the direct impact of ACE was not significant towards the PTG if it stands alone. Resilience was found to become the mediator of individuals experiencing PTG after going through ACE.
IMPLICATION
The result of this research could be a basis for professionals to consider giving counselling to individuals who had gone through ACEs to grow positively. Resilience enhancement, based on the findings that have been previously discussed, has proven to help individuals, who in the process of the crisis, find new meanings in life. These new meanings and the cognitive process will be the ones to drive the emergence of PTG as a superficial psychological function that may increase individuals’ quality of life.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The research discussed had been approved by the Ethics Committee of the Faculty of Psychology, Soegijapranata Catholic University (Approval Number: 005/B.7.5/FP.KEP/IV/2021).
HUMAN AND ANIMAL RIGHTS
No animals were used in the studies that are the basis of this research. All human procedures were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
All the participants gave their written informed consent.
AVAILABILITY OF DATA AND MATERIALS
The authors confirmed that the data supporting the findings of this study are available within the article.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

