All published articles of this journal are available on ScienceDirect.

Eudaimonic Well-Being as a Moderator of the Relationship between Depressive Symptoms and Life Satisfaction
Abstract
Aim
This study aimed to investigate the potential protective role of eudaimonic well-being in mitigating the adverse effects of depressive symptoms.
Background
The dual continua model conceptualizes mental well-being and mental illness as related yet independent dimensions. According to this framework, well-being can serve as an active defense against mental illness.
Objective
Building on the dual continua model, the study aimed to investigate the relationship between depressive symptoms and life satisfaction and the potential moderating role of eudaimonic well-being.
Methods
This hypothesis was tested using a national sample of 17,357 people from 8,162 households in South Korea. Bayesian multi-level modeling was used for data analysis.
Results
The results showed that eudaimonic well-being moderated the relationship between depressive symptoms and life satisfaction. Depressive symptoms were found to have a significant negative effect on life satisfaction in individuals with low and moderate eudaimonic well-being. However, in individuals with high eudaimonic well-being, depressive symptoms had no significant effect on life satisfaction.
Conclusion
These results suggest that eudaimonic well-being plays an important role in mitigating the effects of depressive symptoms on life satisfaction.
1. INTRODUCTION
As global connectivity and technological advancement have led to increasingly complex societal dynamics, the psychological pressures and stressors faced by individuals have also diversified. This complexity has coincided with a prevalence of mental health problems, e.g, symptoms of depression. Depression is recognized as a persistent public health issue in South Korea [1]. According to a study [2], the prevalence of depression in South Korea has been increasing in recent years, particularly among older adults and women. The rate of depression increased from 2.8% in 2002 to 5.3% in 2013 in the nation, highlighting the need for greater attention to depression and its consequences. Given the increasing prevalence of depression, it is crucial to identify psychological factors that can mitigate its psychological toll. This study focuses on eudaimonic well-being as a potential buffer against depressive symptoms. In contrast to hedonic conceptions of well-being, which focus solely on subjective happiness or pleasure, eudaimonic well-being emphasizes the cultivation of one's potential, the pursuit of meaningful goals, and a sense of purpose [3]. This broader perspective on well-being offers a valuable tool for countering the negative effects of depressive symptoms and promoting overall mental well-being.
1.1. Dual Continua Model of Mental Health
The Dual Continua Model of Mental Health [4] is a conceptual framework that departs from traditional deficit-oriented perspectives by positing mental health and mental illness as distinct but interrelated dimensions along separate continua. This model delineates two independent yet interlinked continua: the mental illness continuum encompasses psychopathology and diagnostic categorizations, while the mental health continuum encompasses positive psychological functioning and well-being. This framework implies that individuals can experience both mental health and mental illness simultaneously, as these dimensions are not mutually exclusive. In addition, the framework emphasizes the assessment of mental health independent of the presence or severity of mental illness, recognizing that one may experience varying degrees of flourishing in the absence of disorder. Overall, the Dual Continua Model contributes to a nuanced, multidimensional understanding of mental well-being to promote comprehensive assessment and intervention approaches that respond to the complex realities of human psychology [5].
In the dual continua model of mental health, mental illness (e.g., depression) and positive mental health (e.g., life satisfaction) are considered separate continua rather than a single continuum [6, 7]. Mental illness and positive mental health interact with each other in various ways. For example, one of the sources of information people draw upon when evaluating their lives is their current or recently experienced mood [8], and thus, symptoms of mood disorders or experienced negative affect can significantly influence these evaluations. Empirical evidence shows that mood disorders or negative affect are important negative predictors of life satisfaction [9, 10]. However, the relationship between negative mood and life satisfaction is moderated by various factors. For example, self-efficacy in dealing with anger attenuates, and neuroticism strengthens the association between negative affect and life satisfaction [11, 12].
The Dual Continua Model's distinctive approach to understanding mental well-being and mental illness as related yet separate entities represents a paradigm shift in how we conceive of well-being. Rather than viewing mental well-being as merely the absence of mental illness, this framework positions positive functioning and well-being as proactive defenses against mental illness [1, 9]. The current study, which looks at the possible buffering effects of eudaimonic well-being, has a theoretical basis in the salutogenic approach of this model, which emphasizes cultivating well-being as a means of preventing mental illness. By examining the role of eudaimonic well-being in mitigating the impact of depression on life satisfaction, the current study builds on the core tenet of the Dual Continua Model, which regards positive well-being as an active counterbalance to the burden of mental illness.
1.2. Eudaimonic Well-being as a Moderator
The biopsychosocial model of health suggests that psychological factors play an important role in coping with and recovering from mental illness and trauma [13]. One such psychological factor is eudaimonic well-being, which consists of positive qualities, skills, and attitudes (e.g., purpose in life, competence, good relationships, and a sense of personal growth) that facilitate daily functioning [14, 15]. Eudaimonic well-being, with its emphasis on self-actualization, meaning, and development, may act as a moderator of the adverse effects of depressive symptoms. Existing research suggests that individuals with high levels of eudaimonia may have reduced vulnerability to depressive symptoms and increased psychological resilience [9]. Several mechanisms may underlie this effect. First, engaging in identity-congruent, meaningful, and value-oriented activities may cultivate a sense of purpose and fulfillment, thereby acting as a buffer against depressive symptoms [16]. Second, eudaimonic lifestyles often involve social embeddedness and affiliative bonds [15], which are essential for protection against depression and psychological resilience [17]. The satisfaction of needs for affiliation and connection and the perceived availability of socio-emotional support are protective factors in the face of life adversities. Finally, eudaimonic well-being correlates with adaptive coping strategies [18, 19] that focus on constructive appraisals and problem-focused coping, which can mitigate maladaptive thought patterns associated with the onset of depression [20]. Not only does eudaimonic well-being act as a buffer against depressive symptoms, but research has also shown that treatments that promote eudaimonic well-being can lead to better long-term outcomes for individuals struggling with depression beyond just symptom relief [21].
On this basis, the present study predicted that eudaimonic well-being would moderate the association between depressive symptoms and life satisfaction. This prediction is based on empirical evidence that elements of eudaimonic well-being (such as meaning in life and competence) prevent and facilitate recovery from mental disorders, including depression. For example, Psarra and Kleftaras [22] investigated that perceptions of meaning in life were protective against depression in people with physical disabilities. Another study of a sample of chronically depressed veterans found that life meaning was associated with lower hopelessness and recovery from a depressive episode four months later [23]. A psychotherapeutic strategy focused on increasing eudaimonic well-being (referred to as well-being therapy) has proved useful in managing the residual phase of mood and anxiety disorders [24].
Moreover, this study hypothesized that increased levels of eudaimonic well-being attenuate the correlation between depressive symptoms and life satisfaction. Individuals with higher eudaimonic well-being were predicted to be less affected by depressive symptoms in their overall well-being. By promoting elements of eudaimonic well-being, such as meaningfulness, competence, supportive relationships, and personal growth, people with depression can achieve better mental health and higher life satisfaction, even when depressive symptoms are present. This highlights the potential of eudaimonic well-being as a valuable resource for coping with depressive symptoms and preventing future depressive symptoms. Age, gender, and educational level were also included as control variables in the analysis, considering that substantial evidence from previous studies has demonstrated significant associations between these factors and mental well-being, as well as depressive symptoms [25-27].
2. METHODS
2.1. Participants
The data are from the Koreans’ Happiness Survey 2021, conducted annually by the National Assembly Futures Institute (www.nafi.re.kr/english/index.do), starting in 2020. The target population of the study is individuals aged 15 years or older who currently reside in South Korea and know the Korean language. The survey population consists of households and their members within Statistics Korea's counting districts as of June 30, 2019. The survey employed a stratified sampling method based on region, township and district, and housing type. A total sample of 17,357 respondents (female = 51.7%, Mage = 49.50, SDage = 17.627) was used from 8,162 households. The distribution varied by age group. Individuals aged 66 years and older represented the largest group (32.2%, n=5593), followed by those aged 50-59 years (21.0%, n=3646), and those aged 40-49 years (16.0%, n=2777). The remaining age groups (15-19, 20-29, and 30-39 years) each contributed less than 15% of the total sample. The smallest age group in the sample was 15-19 years old (n=820, 4.7%). The gender distribution by age is shown in Table 1. There was no missing data. No participant was excluded. The survey was completely in Korean. The data are publicly available.
| - | Age Group | Total | ||||||
|---|---|---|---|---|---|---|---|---|
| 15-19 | 20-29 | 30-39 | 40-49 | 50-59 | 60- | |||
| Gender | Male | 416 | 1094 | 1181 | 1362 | 1694 | 2632 | 8379 |
| Female | 404 | 1112 | 1134 | 1415 | 1952 | 2961 | 8978 | |
| Total | 820 | 2206 | 2315 | 2777 | 3646 | 5593 | 17357 | |
2.2. Measures
2.2.1. Life Satisfaction
The satisfaction with life scale [28] was used to measure general life satisfaction, as the main outcome of this study (1 = strongly disagree to 7 = strongly agree). This scale is a brief, five-item measure designed to assess global judgments of an individual's life satisfaction. A sample item is “I am satisfied with my life.” A principal axis factoring analysis of the five items showed that a one-factor structure is consistent with the data, initial eigenvalue = 3.552, extraction sums of squared loadings total = 3.198, explained variance = 63.962%, range of factor loadings = .708 and .842. The Cronbach's alpha was .896.
2.2.2. Eudaimonic Well-being
Three items were used in the survey to measure the eudaimonic aspects of well-being. The items translate as “1- Overall, I feel that many things I usually do in my life are meaningful”, “2- I generally feel a sense of accomplishment from what I do”, “3- I'm free to decide how to live” (0 = do not agree at all to 10 = strongly agree). These questions are based on the questions suggested in OECD’s [29] guidelines for measuring eudaimonic well-being. A principal axis factoring analysis of the three items showed that a one-factor structure is consistent with the data, initial eigenvalue = 2.362, extraction sums of squared loadings total = 2.052, explained variance = 68.386%, range of factor loadings = .765 and .874. The Cronbach's alpha was .864.
2.2.3. Depressive Symptoms
Participants reported the frequency of experiencing five symptoms in the past two weeks: “Irritability and anxiety,” “Unable to stop or control worries,” “Feeling depressed or hopeless,” “Little interest or fun in doing things,” and “Loneliness” (1 = Never to 4 = Almost every day). A principal axis factoring analysis of the five items showed that a one-factor structure is consistent with the data, initial eigenvalue = 3.138, extraction sums of squared loadings total = 2.683, explained variance = 53.653%, range of factor loadings = .658 and .791. The Cronbach’s alpha was .851.
2.5. Data Analysis
The data used here has a nested structure, meaning individuals are nested within families. This is because the data were collected from multiple people within the same family unit. Traditional statistical methods (multiple regression) assume data points are independent, but in this case, family members might share similar experiences or environments that could influence their responses. Multilevel modeling takes this nested structure into account [30]. It allows us to analyze the data while considering the potential influence of grouping on the results, and the dependence of family members. The analysis was conducted in Mplus using a Bayesian estimator with noninformative priors. Noninformative priors were employed because there was no definitive prior knowledge about the parameters. This allows the data itself to drive the conclusions, minimizing potential bias introduced by inaccurate prior assumptions [31]. Two Markov chain Monte Carlo chains were run using the GIBBS (PX1) algorithm and 5000 draws (the first half was used as burnin). The draws were thinned at every 10th iteration. A random intercept model was tested with no group-level covariates. Continuous covariates (eudaimonism, depressive symptoms, age, and education) were group-mean centered [32]. The potential scale reduction factor (PSRF) [33] was used to assess the convergence of the chains to the posterior distribution. The PSRF of the model was 1.000, indicating satisfactory convergence [34]. The Bayesian trace and autocorrelation plots showed optimal chain mixing and acceptable autocorrelation [35]. The Posterior Predictive P-value of the model was 0.474, suggesting an acceptable fit.
3. RESULTS
The correlation matrix for all continuous variables is shown in Table 2. The results of multilevel modeling are shown in Table 3. Except for gender, all covariates were significant predictors of life satisfaction and explained approximately 21% of its individual-level variance (R2 = 0.212). The interaction of eudaimonic well-being and depressive symptoms was also a significant predictor of life satisfaction, suggesting that eudaimonic well-being moderates the association between depressive symptoms and life satisfaction. This interaction is illustrated in Fig. (1). As can be seen, there is a negative association between depressive symptoms and life satisfaction at low and moderate levels of eudaimonic well-being, but there is no significant relationship between depressive symptoms and life satisfaction at high eudaimonic well-being. More specifically, the red line in the figure shows the effect of depressive symptoms on life satisfaction (y-axis) over the range of eudaimonic well-being (x-axis). The blue lines show the credible intervals for the effects. The higher the value of eudaimonic well-being, the weaker the relationship between depressive symptoms and life satisfaction. The credible intervals for all values of eudaimonic well-being (centered) below 1 did not include zero (y-axis), indicating that the effect is negative and significant at low and medium values of eudaimonic well-being. However, the credible intervals included zero after the eudaimonic well-being value of 1, indicating that there is no significant relationship between depressive symptoms and life satisfaction at high levels of eudaimonic well-being.
4. DISCUSSION
The study revealed a remarkable resilience to the adverse impacts of depressive symptoms among individuals exhibiting high eudaimonic well-being. Interestingly, participants with high eudaimonic well-being demonstrated no influence of depressive symptoms on their overall life satisfaction. Conversely, those with lower eudaimonic well-being experienced a notable decrease in life satisfaction due to depressive symptoms. How does eudaimonic well-being protect against depressive symptoms? Eudaimonic well-being is comprised of a range of skills and capabilities that are known to promote resilience [36]. This aspect of well-being is characterized by self-realization, personal growth, and a sense of purpose, which have been found to enhance individuals' capacity to cope with adversity and maintain overall mental health. Individuals who exhibit high levels of eudaimonic well-being are, therefore, likely to be better able to cope with life challenges and the resulting negative moods. Furthermore, individuals with higher levels of eudaimonic well-being are more likely to find meaning in life challenges [37]. Eudaimonic well-being provides psychological resources for coping with difficulties in daily life and stressful events (e.g., [18]). For example, researchers found that people with high eudaimonic well-being tend to view difficult life experiences as transformative [38].
| - | Eudaimonic | Life Satisfaction | Depressive Symptoms | Age |
|---|---|---|---|---|
| Eudaimonic well-being | -- | - | - | - |
| Life satisfaction | .746 | -- | - | - |
| Depressive symptoms | -.313 | -.263 | -- | - |
| Age | -.140 | -.125 | .031 | -- |
| Education | .204 | .209 | -.031 | -.603 |
| Predictor | Unstandardized | 95% Credible Interval | Standardized | ||
|---|---|---|---|---|---|
| Low | Up | Sig | |||
| Eudaimonic well-being (A) | 0.360 | 0.349 | 0.372 | * | 0.434 |
| Depressive symptoms (B) | -0.181 | -0.215 | -0.148 | * | -0.073 |
| A × B | 0.113 | 0.060 | 0.164 | * | 0.044 |
| Female | 0.007 | -0.010 | 0.023 | - | 0.006 |
| Age | 0.002 | 0.001 | 0.002 | * | 0.031 |
| Education | 0.015 | 0.003 | 0.027 | * | 0.018 |
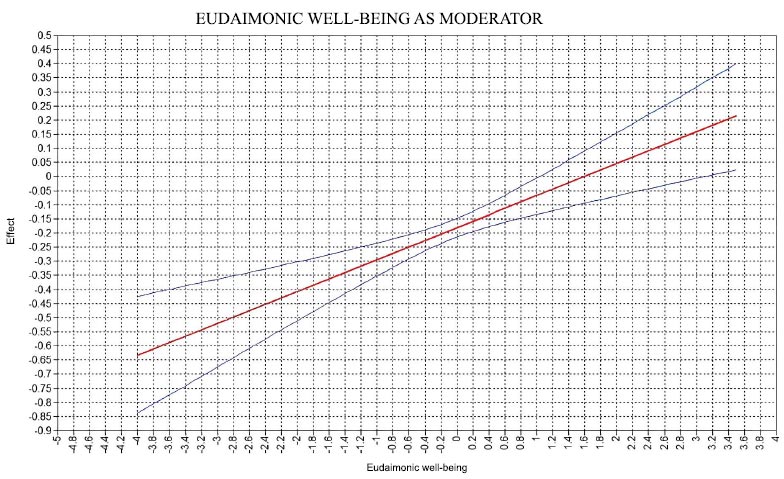
Eudaimonic well-being (centered) as a moderator of the association between depressive symptoms and life satisfaction.
It appears that people with more positive psychological skills are better able to cope with depressive symptoms and do not rely as much on their mood to assess the quality of their lives. For example, they may view depressive symptoms as less harmful, more bearable, and even transformative experiences with some positive outcomes in the future [39]. Overall, this suggests that eudaimonic well-being contributes to the management of depressive symptoms. Therefore, eudaimonic well-being may be considered an asset for promoting adjustment and resilience. A recent longitudinal study spanning 16 years found that eudaimonic well-being protects against future increases in depressive symptoms [9].
The results of this study suggest that promoting eudaimonic well-being may also be a useful goal in the treatment of depressed individuals. Interventions to promote eudaimonic well-being may help reduce the negative impact of depressive symptoms on life satisfaction. Evidence suggests that interventions to promote eudaimonic well-being can indeed be used to protect against and control depressive symptoms [40]. In an eight-week program to promote eudaimonic well-being through facilitated group sessions in community settings and home exercises, it was found that participants showed significant and sustained decreases in depressive symptoms, anxiety, and hostility [41]. This highlights the importance of promoting psychological resources to cope with difficulties in daily life and stressful events and the resulting low mood. For this reason, it might be necessary to concentrate on practices that encourage constructive psychological traits like self-compassion, resilience, and mindfulness. This could include exploring the underlying mechanisms and potential for using eudaimonic well-being as a predictor of depression risk.
While eudaimonic well-being shows promise as a protective factor against depressive symptoms, it is important not to overstate its role in treatment. Depression is a complex, multifaceted disorder with a diverse range of causes that span biological, psychological, and social domains. Effective intervention requires a personalized, multifaceted approach that addresses all of these factors. Although eudaimonic well-being alone may not be sufficient to address the full complexity of depression, cultivating it as part of a comprehensive treatment strategy may help to increase resilience and reduce the psychosocial burden of the disorder. Thus, while eudaimonic living is not a cure-all, it is a valuable consideration in the broader treatment landscape for depression.
The study has several limitations that should be considered when interpreting its results. First, the sample used in this study is from a single population, and it is uncertain whether the results can be generalized to other populations with different demographic, cultural, and lifestyle characteristics. Further studies involving a broader range of populations are needed to test the generalizability of these findings. Second, the study was based on self-report, which may be biased due to social desirability and memory effects. It is possible that participants may have described their experiences in ways that cast them in a more positive light. This raises questions about the accuracy of the self-reports collected. Third, the study used cross-sectional data, which makes it difficult to establish causality among the variables examined. For example, it is not possible to determine whether life satisfaction affects depressive symptoms or whether the relationship is inverse. Longitudinal and/or experimental studies are needed to determine the direction of causality between variables. The study used brief measures to assess eudaimonic well-being and life satisfaction, and these measures may not capture all aspects of these constructs. Further studies are needed to explore other aspects of these constructs with multidimensional measures.
Last but not least, the COVID-19 pandemic, a worldwide public health emergency that significantly impacted many facets of human existence, coincided with the data collection for this study. Empirical evidence suggests that the pandemic exacerbated mental health problems worldwide, with studies reporting increased rates of anxiety and mood disorders [42, 43]. Given the pervasive nature of the pandemic, it is reasonable to assume that at least some participants were affected by adverse effects associated with COVID-19, such as social isolation, physical distancing measures, quarantine protocols, and potential infection. These factors may have had an impact on the mental health and well-being of participants, potentially influencing their responses and, consequently, the results of the study. It is essential to acknowledge the potential impact of pandemic-related factors on the study's outcomes. However, the extent to which these pandemic-related factors influenced the results remains unclear, and there is no straightforward method to distinguish the pandemic's influence on the findings.
CONCLUSION
In conclusion, the study aimed to investigate the relationship between depressive symptoms and life satisfaction and how eudaimonic well-being may influence this relationship. The results of multi-level modeling showed that eudaimonic well-being moderated the relationship between depressive symptoms and life satisfaction, and confirmed the hypothesis that individuals with higher eudaimonic well-being would exhibit a weaker relationship between depressive symptoms and life satisfaction. These findings suggest that eudaimonic well-being may play an important role in mitigating the negative impact of depressive symptoms on life satisfaction. The findings of this study underscore the significance of integrating eudaimonic well-being into intervention strategies for mood (and potentially other types of) disorders.
AUTHORS' CONTRIBUTIONS
It is hereby acknowledged that all authors have accepted responsibility for the manuscript's content and consented to itssubmission. They have meticulously reviewed all results and unanimously approved the final version of the manuscript.
ABBREVIATION
| COVID-19 | = Coronavirus Disease of 2019 |
ETHICAL STATEMENT
Since this is a secondary analysis of already published data, ethical approval was not necessary. No new participant data was gathered. For more information on data collection and study procedures, see https://kossda.snu.ac.kr/handle/20.500.12236/25638.
CONSENT FOR PUBLICATION
This study utilizes a de-identified and publicly available data set. Informed consent was obtained from all participants.

