All published articles of this journal are available on ScienceDirect.

Short Imagery Rescripting Intervention Effects on Non-Suicidal Self-Injury College Students: A Randomized Controlled Trial
Abstract
Background and Objective
Imagery rescripting intervention has proven effective in reducing PTSD. We developed a four-session short intervention to treat non-suicidal self-injurious behaviors. We aimed to examine whether a short imagery rescripting intervention reduces the level of catastrophizing, emotional dysregulation, depression and non-suicidal self-injurious behaviors, and dysfunctional schema modes in non-suicidal self-injurious college students.
Methods
Twenty-six college students with experience of non-suicidal self-injury behaviors were recruited for participation. Participants were randomly assigned to complete the short imagery rescripting intervention group (n = 13) or no treatment control group (n = 13) for 4 weeks. The level of catastrophizing, emotional regulation difficulties, depression, and non-suicidal self-injurious behaviors, and the level of schema modes (vulnerable child, impulsive child, angry child, detached self-soother, detached protector) were assessed before and after the intervention.
Results
The levels of catastrophizing, emotional dysregulation, depression, and the frequency of non-suicidal self-injurious behaviors decreased after the individual short imagery rescripting interventions. The levels of vulnerable child schema mode and impulsive child schema mode decreased after the individual short imagery rescripting interventions.
Conclusion
The individual imagery rescripting intervention was found to reduce the level of cognitive catastrophizing thinking, emotional dysregulation, depression, and the frequency of non-suicidal self-injurious behavior in non-suicidal self-injury college students. These findings suggest that they confirm the efficacy of individual short imagery rescripting interventions in schema therapy, and the individual imagery rescripting intervention will be useful for interventions for non-suicidal self-injurious behavior in young adults counseling and psychotherapy setting.
1. INTRODUCTION
Non-suicidal self-injurious behavior is the act of directly and intentionally damaging a part of one's own body without the intention of suicide [1]. Non-suicidal self-injury, according to the DSM-5 [2], is a diagnostic condition that needs more research. It is defined as “intentionally inflicting behaviors on the body surface that cause bleeding, wounds, or pain on five or more days in the past year, with the intent to engage in self-injurious behaviors that may cause mild or moderate physical damage, i.e., no suicidal intent.” It is the strongest predictor of suicidal behavior among other predictors of suicidal behavior, including depression, hopelessness, post-traumatic stress disorder, and childhood abuse [3]. Non-suicidal self-injurious behavior is violence directed at oneself, most often to regulate emotions [4, 5], and most commonly to relieve severe emotional distress, such as sadness, guilt, flashbacks, and depersonalization [6].
Following non-suicidal self-injurious behaviors, both women and men feel anger, guilt, and shame [7]. Non-suicidal self-injurious behaviors can appear as a motive to reduce or eliminate negative emotions such as anger and stress and perceptions of suicidal thoughts or traumatic memories [8]. In addition, non-suicidal self-injurious behaviors can be used as a self-punitive means or provide a sense of internal control [9].
Non-suicidal self-injurious behaviors typically begin in adolescence and early adulthood [10], with intensification or, conversely, cessation in the late teens to mid-20s [11]. 35-72% of adults who experienced non-suicidal self-injurious behaviors in early adulthood continue to self-injury [12, 13], which is associated with unique characteristics due to the demands of various social roles, such as identity exploration, instability, and feeling trapped in the process of growing into an adult [14]. Depression and anxiety are risk factors for non-suicidal self-injurious behavior [15, 16], and youth with high levels of anxiety and depression are at higher risk for self-injurious behavior [2]. Shinn [17] cited increased indicators of depression or anxiety as a covert sign of non-suicidal self-injurious behavior. A recent study found that more than one-third of college students with major depression have experienced non-suicidal self-injury [18]. Preventive counseling and proactive counseling interventions for psychological difficulties are even more necessary for adolescents as they undergo physical, psychological, and social changes, and this is very relevant to the psychological health of college students in their early adulthood..
Schema Therapy proposes that psychological symptoms, disorders, and problems are caused by the development of maladaptive schemas due to the unmet core childhood needs, such as attachment, in the childhood environment, along with the child's tempera- ment, and that schema modes are triggered when these maladaptive schemas are activated [19]. There are four basic categories of schema modes: innate child modes, dysfunctional critic modes, maladaptive coping modes, and healthy modes. In schema therapy, the goal of treatment from a schema-mode perspective is to develop a healthy adult mode [20].
Imagery rescripting in schema therapy is used to strengthen the healthy adult mode, care for the vulnerable child mode, overcome dysfunctional coping modes and learn new ways of relating [21]. In schema therapy, imagery rescripting uses imagery to allow the self to appear in the image and re-experience past interpersonal traumatic events. Emotional reconnection can be experienced by identifying previously unmet emotional needs and making contact with a vulnerable child. At this point, the emotional needs are met with the experience of a healthy adult mode (either the therapist or the healthy adult mode part of the self), and the distorted cognitive processes can be changed and adaptively restructured to support healthy, rational thinking [22, 23]. Imagery rescripting in schema therapy can more easily access images or imagined events based on traumatic memories through emotionally activated images and rescript them to derive new meaning related to the trauma [24, 25]. Imagery rescripting is more effective than exposure therapy when targeting non-fear-based emotions such as anger, guilt, and shame [26, 27] and has lower participant dropout rates [28]. Imagery rescripting in schema therapy helps clients overcome dysfunctional coping modes such as avoidance and overcompensation and learn new ways of relating [21], providing corrective emotional experiences, satisfying needs, and strengthening healthy adult mode [29].
Arntz and Weertman [30] developed an imagery rescripting protocol that consists of three main steps. Stage 1 is recalling memories from childhood. The client is asked to recall a childhood event associated with an early maladaptive schema and describe it in detail in the child's first-person present tense. In the second stage, the client rescripts the image of the client as a healthy adult. In other words, the client enters the image as a healthy adult and then rescripts the image to protect the child (the client himself) and provide comfort to the child. If the client has difficulty rescripting the image directly, a significant other (e.g., supporter, police officer, therapist, etc.) can take on this role, or the therapist can assist by providing additional coaching for the client's healthy adult self. The third stage is to re-experience the rescripting as a child. The client re-experiences the rescripted image from a child's perspective, becoming aware of what it feels like to be protected and cared for by an adult. In addition, clients can be encouraged to see whether the rescripted image meets their needs and to imagine the changes needed to achieve them. Afterwards, the client experiences a rescripted image with additional changes added from the child's perspective. To investigate the psychological mechanisms underlying non-suicidal self-injurious behavior in college students, Bang [31] selected 430 non-suicidal self-injury college students to examine the mediating effects of dysfunctional schema modes, catastrophizing, emotional dysregulation, and depression on the relationship between negative parent-child relationships in childhood relationships and non-suicidal self-injury. The results showed that negative parent-child relationships in childhood directly influenced depression and non-suicidal self-injurious behaviors and indirectly influenced non-suicidal self-injurious behaviors through the multiple mediating pathways of dysfunctional schema-modes (angry child, impulsive child, punitive critic, detached protector, and detached self-soother), catastrophizing, emotional dysregulation, and depression.
In this study, we aim to examine whether individual short imagery rescripting intervention based on Arntz and Weertman's [30] imagery rescripting protocol reduces levels of variables that have been identified as psychological mechanisms of non-suicidal self-injurious behavior in college students [31]. That is, through this study, we examined whether the individual imagery rescripting intervention in schema therapy significantly changes the level of catastrophizing, emotional dysregulation, depression, and non-suicidal self-injurious behaviors of non-suicidal self-injury college students and whether the individual imagery rescripting intervention in schema therapy significantly changes the level of schema modes (vulnerable child, impulsive child, angry child, detached self-soother, detached protector, punitive critic, and demanding critic) of non-suicidal self-injury college students.
2. METHODS
2.1. Participants and Procedures
This study was conducted with university students who expressed their willingness to participate in the study after being explained how to participate in this study, the procedure for conducting it, and the rights of participants. Recruitment began in April 2023 and was finalized in May 2023. One hundred and twenty-seven undergraduate students at K University in Gyeongsangnam-do partici- pated in the study, and the non-suicidal self-injurious behavior, emotional dysregulation, catastrophizing, and depression scales were administered to them. Before the survey was administered, participants were informed that they could stop the survey at any time if they felt uncomfortable during the survey process and were provided with the researcher's contact information and the contact information of organizations that could help them if they continued to feel uncomfortable after the survey.
Factors that threaten the internal validity of an experiment, which is the ability to conclude that the results of an experiment are due purely to the experimental treatment and not to other factors, include history (personal experience), maturation, test administration, instrument use, statistical regression, subject selection, subject dropout, and subject selection-maturation interactions [32]. History (personal experience), maturity, and test administration can be controlled by including an appropriate control group, statistical regression can be controlled by including a control group selected by the same criteria, and subject selection and subject selection-maturity interactions can be controlled by using random assignment to form groups [33]. In this study, a control group was included in addition to the experimental group, and the experimental and control groups were organized through random assignment to ensure the internal validity of the experiment.
As a screening question, the Self-Injurious Functioning Assessment was used to determine the presence or absence of checks on the frequency and method of self-injury questions and the presence or absence of checks on non-suicidal self-injurious behavior in the past year based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). We then selected university students who reported self-injury on the Non-Suicidal Self-Injury Scale, volunteered to participate in the study, and left their contact information. We prioritized college students who had self-injury within the past year and for more than five days. We did not explain to the selected participants which questions led to the final selection and briefly explained the purpose of the study. This was done to avoid the effect of participants' expectations related to non-suicidal self-injury that may have been created by references to suicidal self-injury.
Thirty participants were initially selected, but four of them withdrew from the study before the start of the study, resulting in a total of 26 participants: 13 in the experimental group and 13 in the control group. To do this, four graduate students unrelated to the study randomly drew slips of paper numbered from 1 to 26 and randomly assigned 13 participants each to the experimental and control groups.
The imagery rescripting intervention was administered to the intervention group (13 participants) from June 2023 to August 2023 on an individualized basis. At the end of each of the four sessions, the participants in the experimental group were briefly informed that the purpose of the study was to investigate the effectiveness of the imagery rescripting intervention. For the control group (waiting list), two sessions of group counseling (4 hours per session) were prepared, but the group counseling could not be conducted due to the personal circumstances of the participants, as the study was conducted during the school final exams and vacations. We attempted to contact the individuals in the control group again to reschedule, but this was not possible.
The imagery rescripting intervention was administered by the first researcher, a doctoral candidate in counseling psychology who completed a 150-hour Schema Therapy counselor training course (Korean Schema Therapy Therapist, Level 2) and is currently practicing as a Korean Schema Therapy Therapist, Level 1. During the course of the intervention, the researcher received 50 minutes of weekly supervision in imagery rescripting from two supervisors, a Korean Schema Therapy Therapist, Level 1, and a Korean Counseling Psychologist, Level 1.
The flow chart of this study is shown in Fig. (1) below.
2.2. Ethics
In accordance with the guidelines set forth in the Helsinki Declaration of 1975, as revised in 2013, this study followed ethical protocols and received approval from the Institutional Review Board (IRB) of Kyungnam University in Changwon, South Korea (Approval number: 1040460-A-2023-012). Prior to their participation, informed consent was obtained from all participants, ensuring their voluntary and informed agreement to take part in the study.
2.3. Intervention
The intervention consisted of four individual imagery rescripting sessions. Prior to the imagery rescripting intervention, the study's dependent measures of non-suicidal self-injurious behavior, emotional dysregulation,
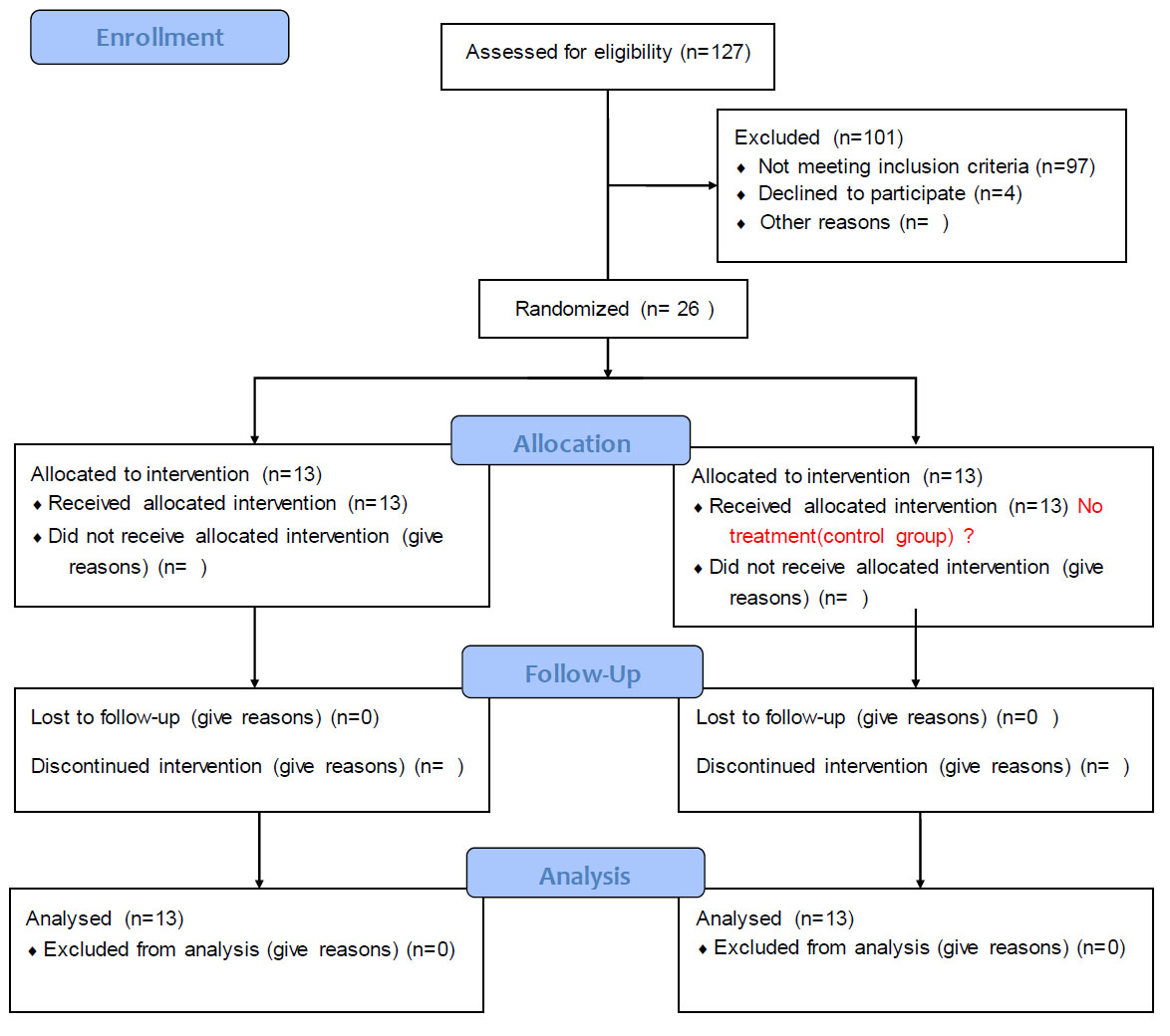
CONSORT participant flow chart.
catastrophizing, depression, and schema modes (vulnerable child, angry child, impulsive child, punitive critic, demanding critic, detached protector, and detached self-soother) were measured. The imagery rescripting intervention for this study consisted of four sessions, each lasting 50 minutes, for a total of 52 (13 persons×4 sessions) sessions and 2600 (50 minutes ×13 persons×4 sessions) minutes of total time. In this study, based on Arntz and Weertman's [30] three-stage protocol, the intervention consisted of four individual imagery rescripting sessions. Each session was summarized as follows: the first session is to find the hot spot through bonding and imagery drawing; the second session is to reminisce about childhood, which is the hot spot found during the first session; the third session is to rescript the image as a healthy adult; and the fourth session is to re-experience the rescripted image as a child, sharing an overall evaluation of the rescripted image.
2.3.1. First Session
Participants were given a brief explanation of breathing exercises and imagery rescripting in Schema Therapy. They were then asked to imagine a safe place while breathing. They then used imagery rescripting to identify emotional “hot spots” from their childhood that they would work on in session 2. More specifically, the client is asked to think back to their childhood and represent a memorable or thought-provoking event in nine key pictures or words using the mental picture method. After sharing a short story about each event, the client chooses the scene they would like to work on first, or the client and counselor work together to decide which scene to work on in the next session.
2.3.2. Second Session
Participants were guided into an image of the ‘hot spot’ that had been identified last week and explained the situation from the present point of view. At this time, the researcher helped the participants vividly re-experience the scene. Questions using five senses, such as “What do you see now? What do you hear? What do you smell?” or changing the questions to suit the age at which they experienced the scene, such as “Hey, where are you now? Oh, how do you feel now?” It helped them express their emotions as a child and identify unmet needs or help that should have been granted, and if they needed someone else’s help, the researcher entered the scene and helped satisfy the needs of young children in various ways.
2.3.3. Third Session
Participants were asked to enter the scene as adults. The researcher helped them to look at the child in the scene as an adult and to notice what they would like to do for the child as an adult and what they could do for the child as an adult and then helped them to actually do it in the imagery scene. “Where is the child now? What is going through the child's mind right now? How does the child look? How do you feel about the situation right now? How would you like to help the child?” and other questions were asked to help the participant express the vulnerable child mode and allow the participant's healthy adult mode to function.
2.3.4. Fourth Session
Participants were asked to re-imagine the scene as a young child, and following the previous session, the young child in the imaged scene was asked if anything else was needed and helped to request this directly from a healthy adult. After all sessions were completed, time was set aside to listen to the participants' impressions and share them.
2.4. Measures
2.4.1. Functional Assessment of Self-mutilation Scale (FASM)
This study used the 10-item Korean version of the 7-point Likert-type Functional Assessment of Self-mutilation (FASM) developed by Lloyd-Richardson, Kelley, and Hope [34], translated into Korean, and validated by Kwon and Kwon [35]. The internal consistency for FASM in this study was .82 at the pretest and .67 at the posttest.
2.4.2. The Korean Version of the Center for Epidemiologic Studies-depression Scale (CES-D)
This study used 20 items with a 4-point Likert-type Korean version of the Center for Epidemiologic Studies-depression Scale (CES-D), developed by Radloff [36] and validated by Jeon, Choi, and Yang [37]. In this study, the internal consistency for CES-D was .92 at the pretest and .93 at the posttest.
2.4.3. Catastrophizing Scale
This study used the Cognitive Emotion Regulation Questionnaire (CERQ), a 5-point Likert-type scale developed by Garnefski et al. [38], and translated into Korean by Kim [39]. We used only the catastrophizing factor (3 items) from the nine subfactors of the maladaptive cognitive emotion regulation strategies scale. The internal consistency of the catastrophizing scale in this study was .87 at the pretest and .89 at the posttest.
2.4.4. Korean Difficulties in Emotional Regulation Scale(K-DERS)
This study used the Korean version of the Difficulties in Emotional Regulation Scale (K-DERS), which was translated and validated by Choi [40] from the Difficulties in Emotional Regulation Scale (DERS) developed by Gratz and Roemer [41], which consists of a Likert-type 5-point scale. Of the six sub-factors of the emotional dysregulation scale, only four were selected: 'unacceptability of emotions', 'difficulty controlling impulses', 'limited access to emotional regulation strategies', and 'difficulty in goal-directed behavior', and a total of 12 items were used. The internal consistency of the scale in this study was .90 at pretest and .90 at post-test.
2.4.5. Korean Schema Mode Inventory (SMI)
The shortened Korean version of the Schema Mode Inventory (SMI), a six-point Likert-type scale developed by Young et al. [42], translated into Korean, validated, and shortened By Song and Lee [43], was used to measure the child mode (vulnerable, angry, impulsive) and dysfunctional critic mode (punitive critic and demanding critic): (SMI) 61 items, including 15 items from the child mode (5 items from the vulnerable child mode, 5 items from the angry child mode, and 5 items from the impulsive child mode), 10 items from the dysfunctional critic mode (5 items from the punitive critic mode and 5 items from the demanding critic mode), 5 items from the dysfunctional avoidant coping mode (5 items from the detached protector mode), and 5 items from the detached self-soother mode of the 186-item SMI-1-2-Plus translated into Korean and validated by Lee and Song [44]. The internal consistency for SMI subscales in this study was as follows: vulnerable child, pretest.86, posttest.85; angry child, pretest.78, posttest.69; impulsive child, pretest.83, posttest.90; punitive critic, pretest.84, posttest.90; demanding critic, pretest.83, posttest.84; detached protector, pretest.78, posttest.85; detached self-soother, pretest.84, posttest.84.
2.5. Statistical Analyses
To ensure the homogeneity of the treatment (intervention) and no-treatment (wait-list control) groups, we compared demographic characteristics across groups and tested for between-group differences in the pre-measured measures. To test the significance of the mean difference between the experimental and control groups, we conducted a mixed ANOVA, where the two confounding variables (between and within groups), which are not captured by the independent group design, are decom-
| Variables | Intervention Group M (SD) |
Control Group M (SD) |
t | p |
|---|---|---|---|---|
| Catastrophizing | 12.85 (3.76) | 10.00 (4.71) | 1.70 | .10 |
| Emotional Dysregulation | 39.07 (7.61) | 34.31 (9.53) | 1.39 | .18 |
| Depression | 26.62 (13.09) | 23.08 (11.36) | .74 | .47 |
| Non-Suicidal Self-Injurious behaviors | 13.00 (12.70) | 7.62 (9.29) | 1.23 | .23 |
| Variables | Intervention Group M (SD) |
Control Group M (SD) |
t | p |
|---|---|---|---|---|
| Vulnerable Child | 15.92 (5.47) | 15.08 (6.41) | .36 | .72 |
| Angry Child | 14.31 (5.51) | 13.38 (4.52) | .47 | .65 |
| Impulsive Child | 14.15 (3.18) | 13.38 (5.82) | .42 | .68 |
| Detached Protector | 13.00 (4.88) | 13.62 (5.44) | -.30 | .76 |
| Detached Self-Soother | 19.15 (5.29) | 19.46 (6.98) | -.13 | .90 |
| Punitive Critic | 8.85 (3.60) | 10.69 (5.30) | -1.04 | .31 |
| Demanding Critic | 18.15 (6.22) | 20.00 (6.18) | -.76 | .46 |
posed and clarified by the within-group design. In addition, partial η2 was calculated to determine the effect size of each variable on the change in the level of each measure and schema mode scale in order to more clearly identify the effect of the imagery rescripting intervention on the experimental group. Partial η2 is the proportion of the total variation that can be attributed to the effect of the treatment on the experimental population, with no treatment effect at the .01 level, a moderate treatment effect at the .06 level, and a large effect at .14 or higher [39].
3. RESULTS
3.1. Test the Homogeneity of Variances between Groups
To ensure that the individual rescripting treatment (intervention) and no-treatment (control) groups were homogeneous, we compared the demographic character- istics of the groups prior to the rescripting intervention and tested for between-group differences on the pre-measurements. Both gender (χ2=2.78, p=.10) and age (t=.40, p=.69) didn’t make significantly different between the two groups. Pre-scores on the measurement variables and schema mode inventory scales were also not significantly different between the intervention and control groups, confirming pre-homogeneity of the measurement variables and schema mode inventory scales (Tables 1, 2).
The mean depression score (CES-D) in Table 1 shows that both the intervention and control groups selected as non-suicidal self-injury are above the cutoff score of 21 (Korea) for diagnosis of depression, and when examining individuals in each group, 9 (69.2%) of the intervention group and 7 (53.8%) of the control group are above the cutoff score of 21, indicating that non-suicidal self-injurious behaviors and depression are co-morbid.
3.2. The effect of the rescripting intervention on each measure variable
The results of the mixed ANOVA analyses to test for differences in score changes on each measure between the intervention and control groups are presented in Table 1. To examine the effect of the individual imagery rescripting intervention on reducing participants' levels of each measure, pre-post test data for each measure scale are presented in Fig. (2).
| Variables | MS | F | p | Partial η2 | |
|---|---|---|---|---|---|
| Catastrophizing | Group | 2.77 | .15 | .71 | .28 |
| Time | 2.77 | .18 | .68 | ||
| Time x Group | 142.23 | 9.23 | .01 | ||
| Emotional Dysregulation | Group | 6.23 | .04 | .84 | .40 |
| Time | 155.77 | 6.50 | .02 | ||
| Time x Group | 376.92 | 15.71 | .001 | ||
| Depression | Group | 42.48 | .19 | .67 | .27 |
| Time | 46.17 | 1.07 | .31 | ||
| Time x Group | 371.56 | 8.63 | .007 | ||
| Non-Suicidal Self-Injurious behaviors | Group | 204.02 | 1.04 | .32 | .05 |
| Time | 5.56 | .24 | .63 | ||
| Time x Group | 26.33 | 1.12 | .30 | ||
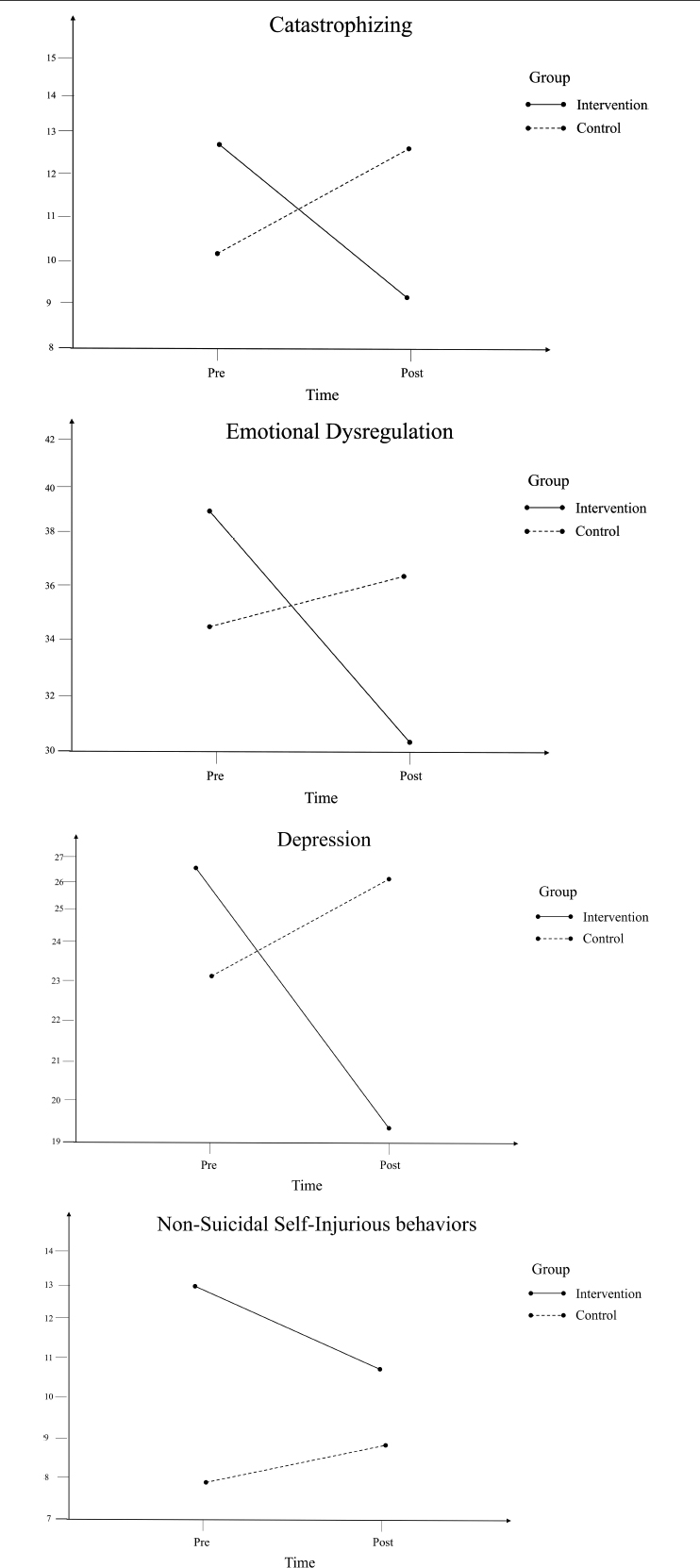
Changes over time for each measure variable in the intervention and control groups.
As shown in Table 3, there were interaction effects between time and group for the variables of catastrophizing (F = 9.23, p<.01), emotional dysregulation (F = 15.71, p<.001), and depression (F = 8.63, p<.01). In other words, there was a statistically significant difference in the degree of change in catastrophizing, emotional dysregulation, and depression between the intervention and control groups. Therefore, it can be concluded that the intervention group had significantly lower levels of catastrophizing, emotional dysregulation, and depression than the control group. In addition, the partial η2, the effect size of the intervention, was greater than.14 [45], which is the threshold for a significant effect.
However, as shown in Table 3, there was no interaction effect between time and group on the non-suicidal self-injurious behavior variable (F = 1.12, n.s.). In other words, there was no statistically significant difference in the degree of change in non-suicidal self-injurious behavior between the intervention and control groups. Therefore, it cannot be concluded that the intervention group showed a decrease in non-suicidal self-injurious behavior after the imagery-rescripting intervention compared to the control group.
3.3. Changes in the Frequency of Non-suicidal Self-injurious Behaviors during the Imagery Rescripting Intervention
The frequency of participants' attempts at self-injurious behaviors during the imagery rescripting intervention is shown in Table 4, and the trends of those who attempted self-injurious behaviors are shown in Table 5.
As shown in Table 4, 46.2% (6 participants) did not attempt a self-injurious behavior, and 53.8% (7 participants) attempted a self-injurious behavior during the four sessions (4 weeks) of the imagery rescripting intervention.
As shown in Table 5, 100% (7) of the 7 participants who attempted self-injurious behaviors during the 4 sessions (4 weeks) of the imagery rescripting intervention reported a decrease in the frequency of self-injurious behaviors compared to pre-intervention, and none reported a change or increase in the frequency of self-injurious behaviors compared to pre-intervention. Therefore, the imagery-rescripting intervention was effective in stopping self-injurious behaviors in 46.2% of participants (6 participants) and in reducing self-injurious behaviors frequency in 100% (7 participants) of those who did not stop self-injurious behaviors. In other words, the imagery rescripting intervention was effective in reducing self-injurious behaviors frequency in all 13 participants.
3.4. The Effect of the Rescripting Intervention on each Schema Mode
The results of the mixed ANOVA analyses to test for differences in score changes on each schema mode between the intervention and control groups are presented in Table 6. To examine the effect of the individual imagery rescripting intervention on reducing participants' levels of each schema mode, pre-post test data for each schema mode scale is presented in Fig. (3).
| Attempted Self-injurious Behavior | Frequency | Percent |
|---|---|---|
| Yes | 7 | 53.8 |
| No | 6 | 46.2 |
| Total | 13 | 100 |
| Attempted Self-injurious Behavior Frequency | Number | Percent |
|---|---|---|
| Decreased | 7 | 100 |
| Unchanged | 0 | 0 |
| Increased | 0 | 0 |
| Total | 7 | 100 |
| Schema Modes | MS | F | p | Partial η2 | ||
|---|---|---|---|---|---|---|
| Vulnerable Child | Group | 18.48 | .34 | .57 | .24 | |
| Time | 2.33 | .32 | .58 | |||
| Time x Group | 54.02 | 7.36 | .01 | |||
| Angry Child | Group | 1.56 | .04 | .84 | .02 | |
| Time | .02 | .002 | .96 | |||
| Time x Group | 4.33 | .54 | .47 | |||
| Impulsive Child | Group | 3.77 | .07 | .79 | .18 | |
| Time | 13.00 | 3.10 | .09 | |||
| Time x Group | 22.23 | 5.30 | .03 | |||
| Detached Protector | Group | 27.77 | .64 | .43 | .03 | |
| Time | 15.08 | 2.03 | .17 | |||
| Time x Group | 9.31 | 1.25 | .27 | |||
| Detached Self-Soother | Group | 30.77 | .90 | .35 | .02 | |
| Time | .69 | .02 | .90 | |||
| Time x Group | 19.68 | .40 | .51 | |||
| Punitive Critic | Group | 81.25 | 2.80 | .11 | .03 | |
| Time | .02 | .003 | .96 | |||
| Time x Group | 5.56 | .75 | .39 | |||
| Demanding Critic | Group | 42.28 | 1.02 | .32 | .00 | |
| Time | 6.94 | .23 | .64 | |||
| Time x Group | .02 | .001 | .98 | |||
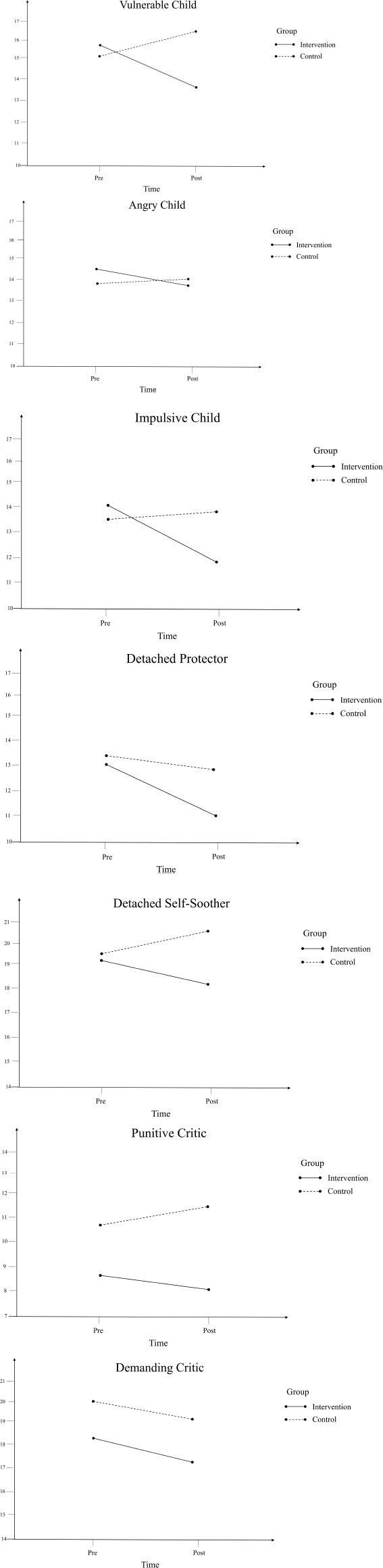
Changes over time for each schema mode in the intervention and control groups.
As shown in Table 6, there were interaction effects between time and group for the modes of vulnerable child (F = 7.36, p<.01) and impulsive child (F = 5.30, p<.05). In other words, there was a statistically significant difference in the degree of change in catastrophizing, emotional dysregulation, and depression between the intervention and control groups. Therefore, it can be concluded that the intervention group had significantly lower levels of vulnerable child and impulsive child mode than the control group. In addition, the partial η2, the effect size of the intervention, was greater than.14 (Kittler et al., 2007), which is the threshold for a significant effect.
However, as shown in Table 4, there was no interaction effect between time and group on the angry child (F =.54, n.s.), detached protector (F = 1.25, n.s.), detached self-soother (F =.40, n.s.), punitive critic (F =.75, n.s.), and demanding critic (F =.23, n.s.) mode. In other words, there was no statistically significant difference in the degree of change in the angry child, detached protector, detached self-soother, punitive critic, and demanding critic mode between the intervention and control groups. Therefore, it cannot be concluded that the intervention group showed an angry child, detached protector, detached self-soother, punitive critic, and demanding critic mode decrease in non-suicidal self-injurious behavior after the imagery-rescripting intervention compared to the control group.
4. DISCUSSION
In this study, we aimed to investigate the effectiveness of schema therapy's imagery rescripting intervention on 26 college students with a history of non-suicidal self-injury. We examined changes in catastrophizing, emotional dysregulation, depression, and non-suicidal self-injurious behaviors from pre- to post-treatment, as well as changes in schema modes. The main findings and implications of this study include the following:
First, the effects of the individual imagery rescripting intervention on each of the measured variables were examined as follows:
(1) The individual imagery rescripting intervention was found to reduce catastrophizing levels in non-suicidal self-injury college students in a randomized controlled trial. These findings are consistent with previous research [46]. Cognitive changes were found during the imagery rescripting intervention process, suggesting that cognitive changes, such as catastrophizing, may be a psychological mechanism that contributes to changes in psycho- pathological symptoms or psychological difficulties, such as PTSD.
(2) The individual imagery rescripting intervention was found to reduce levels of emotional dysregulation in non-suicidal self-injury college students in a randomized controlled trial. These findings are consistent with previous research [47]. During the imagery rescripting intervention, participants may become better able to regulate their emotions by experiencing the fulfillment of their emotional needs with the researcher. Therefore, it is possible that the imagery rescripting intervention reduces the level of emotional dysregulation by fulfilling participants' emotional needs in the mental image, which in turn suggests that the imagery rescripting intervention may improve emotional regulation.
(3) The individual imagery rescripting intervention was found to reduce depression levels in non-suicidal self-injury college students in a randomized controlled trial. These findings are consistent with previous research [48]. They found that the process of the imagery rescripting intervention decreased negative emotions and increased positive emotions. This study also found lower levels of depression, a negative emotion, suggesting that the imagery rescripting intervention may be effective in treating a range of emotional difficulties, including anxiety, not just depression.
(4) In a randomized controlled trial, the effectiveness of the individual imagery rescripting intervention was found to be nonsignificant in reducing self-injurious behavior in non-suicidal self-injury college students. However, 46.2% of participants (6 participants among the 13 participants of the intervention group) stopped self-injurious behaviors during the intervention, and 100% of participants (7 participants among the 13 participants of the intervention group) who did not stop self-injurious behaviors showed a decrease in self-injurious behaviors frequency.
This implies that the imagery rescripting intervention had an impact on reducing self-injurious behavior for all 13 participants. This suggests that the imagery rescripting intervention reduces the frequency of non-suicidal self-injurious behavior in non-suicidal self-injury college students.
Second, the effects of the individual imagery rescripting intervention on each of the schema modes were as follows:
(1) The individual imagery rescripting intervention was found to reduce the levels of vulnerable child mode and impulsive child mode, but not angry child mode, in a randomized controlled trial. The reduction in vulnerable child mode levels is consistent with the therapeutic goal of imagery rescripting to care for the vulnerable child mode, which is to promote a stronger sense of security and healthy attachment [49].
The reduction in the levels of vulnerable and impulsive child mode seems to be in line with the definition of non-suicidal self-injury treatment and its effectiveness as devised by Gratz and Gunderson [50]. According to them, it aims to first recognize, understand, and accept emotions, and second, engage in goal-directed behavior and inhibit impulsive behavior. Impulsivity is a hallmark of the impulsive child mode and is also closely related to impulsivity associated with non-suicidal self-injury in adolescence and early adulthood [51]. Thus, the imagery rescripting intervention was significantly effective for the vulnerable child mode, which is characterized by emotion recognition and acceptance, and the Impulsive Child mode, which is characterized by impulsivity, suggesting that it may be a highly effective therapeutic intervention for non-suicidal self-injury. However, in the case of the Angry Child mode, the therapeutic process of recognizing and expressing one's feelings can be a lengthy one, and the chair technique is suggested to be a very useful treatment for this mode in Schema Therapy [49]. Therefore, it is possible that the four sessions of the imagery rescripting intervention in this study may not have been enough to produce significant effects on the Angry Child mode.
(2) The individual imagery rescripting intervention did not significantly reduce levels of Punitive Critic, Demanding Critic, Detached Protector, and Detached Self-soother in a randomized controlled trial. These findings seem to support the results of Bang [31]. The results of Bang [31] showed that negative parent-child relationships in childhood were positively related to both dysfunctional schema modes, and dysfunctional schema modes were positively related to emotional dysregulation and depression. However, differences were also identified between the Angry Child and Impulsive Child modes, the Demanding Critic and Punitive Critic modes, and finally, the Detached Protector and Detached Self-Soother modes, which each influenced non-suicidal self-injurious behavior through different multi-mediational pathways. Given the different multimodal pathways of these modes, the short-term effects of the imagery rescripting intervention are likely to differ due to the differences in each mode.
In the case of the critic mode, the idea is that this mode is necessary and even requires actual punishment, or nothing will be accomplished. Sometimes, if there is little good parental influence, the person may be so afraid of the dysfunctional critic mode that they resist the idea of having it. In this case, the therapist should be able to address the vulnerable child mode first by acting as a vulnerable child mode [20]. In general, it is rare for a client to feel safe enough to disclose their distress early in therapy, and this is where coping styles such as detached protector and detached self-soother come in to protect themselves [52]. In order to protect themselves, detached protectors and detached self-soothers distance themselves from core vulnerabilities, such as hidden wounds or shame.
In addition, because the detached protector and detached self-soother are characterized by avoidance by blocking out thoughts and feelings that might trigger a psychotic episode, they may also unconsciously avoid therapeutic approaches when they are activated. When these coping modes are strong, the vulnerable child mode is often hidden [53], so it is necessary to address the vulnerable child mode first and use empathic confrontation or limit setting as a therapeutic intervention for the maladaptive coping mode [54]. In the case of detached protector and detached self-soother modes, the triple and quadruple mediation pathways identified in Bang’s study [31] suggest that increased use of various schema therapy therapeutic approaches or sessions, such as mode dialogues, is necessary to significantly reduce levels of critic, detached protector, and detached self-soother modes. These findings are consistent with the understanding of schema modes as cognitive, emotional, and behavioral. This suggests that a slow, in-depth approach may be necessary when dealing with the critic, detached protector, and detached self-soother modes.
5. IMPLICATION
The main significance of this study is as follows: First, it sheds light on the role of unmet childhood needs and associated vulnerable and impulsive childhood modes as underlying Schema Therapy therapeutic mechanisms in non-suicidal self-injury interventions in college students. Second, the imagery rescripting intervention has been shown to reduce catastrophizing thinking, emotional dysregulation, and depressive levels, which are antecedents of non-suicidal self-injurious behaviors [31], as well as the frequency of suicidal self-injurious behavior. Third, the study found differences between the interventions for non-suicidal self-injury among college students. This suggests that the imagery rescripting intervention is highly effective in treating college students with non-suicidal self-injury, but it also suggests that it can be expected to be effective for emotional difficulties or emotional disorders. The findings of this study provide a different perspective on understanding non-suicidal self-injurious behavior in college students by identifying the characteristics of this behavior. It is hoped that these findings will be useful for interventions for non-suicidal self-injurious behavior in adolescence in counseling and psychotherapy settings.
6. LIMITATIONS
The limitations of this study are as follows: First, the therapist in the intervention and control groups was the same as the researcher in this study, so it cannot be ruled out that the researcher's expectation effect may have influenced the results. Therefore, it is necessary to confirm the results by conducting a study with a different therapist and researcher. Second, the participants were limited to college students, which limits the generalizability of the results. Considering that the prevalence of non-suicidal self-injury varies by age, it is necessary to include a wider range of age groups, including late adulthood. Furthermore, adolescents and early adulthood may differ somewhat from school-aged individuals in terms of academic stress, differences in peer group affiliation, and the impact of family environment. These differences may manifest as differences in the currently dominant schema modes and need to be identified. Third, we did not find significant changes in the critic, detached protector, and detached self-soother modes; therefore, it may be worthwhile to adjust the sessions or construct different imagery rescripting interventions, such as a mode dialog using the chair technique or an imagery scene intervention focusing on the critic mode, in addition to the imagery rescripting intervention, to identify changes in these modes. Fourth, the Korean version of the Functional Assessment of Self-mutilation (FASM), a measure of non-suicidal self-injury, asks about the duration of self-injurious behavior in the past year, which may not be adequate to measure changes in non-suicidal self-injurious behavior after four sessions of rescripting. Therefore, other measures of non-suicidal self-injury should be used to determine the effect of imagery rescripting on non-suicidal self-injurious behavior. Fifth, the control group participants in this study were primarily non-suicidal self-injury college students with comorbid depressive symptoms, who volunteered to participate because they desired and required immediate psychological intervention. However, their assignment to the control group, where they did not receive immediate and appropriate intervention, may have caused harm. In addition, the experimental design of this study was planned to have an experimental group and a waiting list control group, so that the control group participants would be withheld from treatment until the experimental group participants were treated, and the treatment would be given to them after the experimental group participants were treated, but this was not possible due to the timing of the intervention coinciding with the university summer vacation. We believe that future intervention studies with students should take these considerations into account when designing experiments. Sixth, this study was not able to follow up after the four sessions to determine if the effects were sustained. In addition, it is believed that non-suicidal self-injurious behavior in adolescents is a long-standing behavior and may be more effectively intervened through long-term imagery rescripting interventions rather than short imagery rescripting interventions. Therefore, future research should take these considerations into account and test the effectiveness of individualized imagery rescripting on non-suicidal self-injurious behavior through longer interventions and follow-up.
CONCLUSION
Taken together, it can be concluded that the individual imagery rescripting intervention in this study reduced the frequency of catastrophizing, emotional dysregulation, depression, and non-suicidal self-injurious behaviors in the participants, and that the individual imagery rescripting intervention, which focused on negative parent-child relationships in childhood, reduced vulnerable and impulsive child modes, thereby influencing negative thoughts, feelings, and behaviors related to childhood complex trauma. In contrast, the control group in this study showed slightly elevated levels of catastrophizing, emotional dysregulation, and depression, suggesting that the environmental change of the start of a new semester at the university may have had an impact, or that cognitive and emotional difficulties may increase in the absence of any therapeutic intervention.
AUTHORS’ CONTRIBUTION
It is hereby acknowledged that all authors have accepted responsibility for the manuscript's content and consented to its submission. They have meticulously reviewed all results and unanimously approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| DSM-5 | = Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition |
| IRB | = Institutional Review Board |
| FASM | = Functional Assessment of Self-mutilation Scale |
| CES-D | = Center for Epidemiologic Studies-depression Scale |
| SMI | = Schema Mode Inventory |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study followed ethical protocols and received approval from the Institutional Review Board (IRB) of Kyungnam University in Changwon, South Korea (Approval number: 1040460-A-2023-012).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee, and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Prior to their participation, informed consent was obtained from all participants, ensuring their voluntary and informed agreement to take part in the study.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
ACKNOWLEDGEMENTS
Declared none.

