All published articles of this journal are available on ScienceDirect.

Quarter-life Crisis: Spiritual Well-being as a Mediator in the Relationship Between Emotion Regulation, Social Support, Religious Activities, and Quality of Life
Abstract
Aims
This research aims to analyze the role of spiritual well-being in shaping quality of life by employing a model based on the framework of the psychological theory.
Background
The transition into early adulthood often brings about periods of uncertainty known as quarter-life crisis, marked by challenges in education, career, and social responsibilities. Identifying the factors that enhance Quality of Life (QoL) is essential for supporting individuals in successfully managing these challenges.
Objective
This study investigated how spiritual well-being mediates the relationship between emotional regulation, social support, religious activities, and QoL during a quarter-life period.
Methods
Using a correlational quantitative design and convenience sampling, we collected data from 255 participants aged 20-30 years using convenience sampling. We analyzed the data using structural equation Modelling (SEM) with measures adapted for the Indonesian context: the Spiritual Well-Being Scale (SWBS), Emotion Regulation Scale, Multidimensional Scale of Perceived Social Support (MPSS), Short Form Health Survey (SF-36), and Religious Activities Scale.
Results
The results showed that emotional regulation, social support, and religious activities significantly influenced QoL, highlighting their importance in shaping positive life perceptions during quarter-life challenges.
Discussion
This study confirms the role of spiritual well-being in promoting the quality of life. Participants who perceived their quality of life as being enhanced through the implementation of emotional regulation, social support, and religious activities demonstrated intentions aligned with spiritual well-being.
Conclusion
It can be concluded that there is empirical evidence for the mediating role of spiritual well-being in the intricate relationship between Emotional Regulation, Social Support, and Religious Activities and QoL among quarter-life crisis. The findings of our study showed that Quality of Life can be achieved effectively through the Spiritual Well-Being internalization process.
1. INTRODUCTION
A quarter of one's life presents a significant challenge for adults. Generally, individuals in the quarter-life phase experience a critical period of emotional and intellectual development due to numerous life stressors [1, 2]. Prior to conducting the study, ethical approval was obtained, and informed consent was gathered from subjects at this transitional age. Data from the Indonesian National Adolescent Mental Health Survey (I-NAMHS) in 2022 indicated that 34.9% of the young generation experienced mental health disorders, with anxiety disorders being the most prevalent at 26.7%, followed by hyperactivity at 10.6%. Depression is ranked the third most common mental health issue in Indonesia at 5.3% [3]. Poor QoL was observed in the mental health domain [4]. The quarter-life stage, comprising the generation born between the mid-1990s and early 2010s in Surakarta, Indonesia, confronts identity exploration and a sense of instability while maintaining optimism about the future in pursuit of an improved quality of life (QoL).
Individuals face unprecedented challenges in establishing their adult identity, career trajectory, and social relationships, which makes QoL a particularly relevant outcome measure. Unlike other life stages, the quarter-life period uniquely combines intense personal development with significant external pressures, creating a distinct impact on the overall quality of life. Research has found that young professionals experiencing quarter-life crises have low psychological well-being, low curiosity, and high perfectionism [5]. Quarter-life crises in early adulthood have a significant impact on mental health [6-8].
During the quarter-life period, meaningful work, perceived value of colleagues, and enjoyment in performing daily tasks significantly predict happiness and quality of life [9]. A few studies [10-12] examined the factors associated with quality of life, including perceptions of roles, health, social support, and strategies for addressing encountered challenges.
High-quality social support during this period is associated with lower levels of depression and some are mediated by gratitude [12, 13]. The initial survey conducted by researchers on 250 respondents across age groups and genders demonstrated that social support had a positive and significant influence on Quality of Life (QoL). Furthermore, researchers have observed that social support exerts a positive influence on the quality of life, which is mediated by Spiritual well-being. The results indicated that social support influenced quality of life by 72.4%. Concurrently, spiritual well-being influences quality of life by 80.9%. Spiritual welfare has been proposed to mediate social support for individuals in the quarter-life age range.
Spiritual Well-being (SWB) represents a compelling mediating variable in quarter-life crisis research because of its fundamental connection to meaning-making processes and existential questioning. Spiritual issues play an important role in the lives of religious individuals, who seek economic, physical, and mental well-being [14]. Researchers have also examined how some therapy needs to improve the spiritual well-being of postgraduate students experiencing a quarter-life crisis, leading to more positive self-assessments and reduced anxiety [15].
The capacity to address crises in adulthood requires enhancement to enable individuals to transform and reassess the significance of each life-stage transition [16]. Nevertheless, younger age is associated with increased negative affect and mental health concerns, and emotion regulation may represent a promising target for interventions [17]. This finding was corroborated by a study, which demonstrated that stress during the early life stages disrupts neurodevelopment and weak character increases the risk of subsequent psychiatric disorders [18, 19].
Transdiagnostic interventions based on emotion regulation could be used to address emotional disorders [20]. Emotional regulation is a critical component that must be developed to prevent or enhance resilience when confronting uncertain situations in daily life. Furthermore, religious practices conducted in everyday life are hypothesized to strengthen an individual's capacity to face diverse challenges [21].
Spiritual well-being is conceptualized as a construct related to the divine, encompassing both purpose and meaning. It reflects an individual's relationship with oneself, others, and a broader entity and is associated with quality of life [22]. Research has demonstrated the influence of spiritual well-being on quality of life in various populations, including elderly individuals residing in nursing homes, visually impaired individuals, and those with physical disabilities [23-26]. The subjects examined in these studies were predominantly in compromised physical condition. The proposed research offers a novel approach by focusing on subjects at the intersection of ages who are in optimal physical condition. This presents an intriguing avenue for investigation, owing to the unique characteristics of this population.
2. MATERIALS AND METHODS
The endogenous variables examined in relation to exogenous variables included emotional regulation, social support, and religious activities. Spiritual well-being was investigated to determine its potential role as a mediator. Structural Equation Modeling (SEM) was employed for data analysis. The sample, randomly selected from individuals aged 20–30 years, will be representative and enable the researcher to generalize the findings to a broader population.
The decision to focus on participants aged 20-30 years was strategically aligned with both theoretical frameworks and empirical evidence regarding quarter-life experiences. This age range captures the critical period when individuals typically navigate significant life transitions and face unique developmental challenges characteristic of quarter-life crises proposed a new developmental stage, namely emerging adulthood, an extended adolescent transitional phase ranging from 18-29 years of age. Arnett's theory is further expanded to find the phenomenon of quarter-life crisis, a phenomenon of anxiety about the future by 20-year-old adolescents who form independence both financially and in romantic relationships [26-29]. This study used the population from the quarter-life age group of the Surakarta Residency.
2.1. Data Collection
Participants were selected using convenience sampling, comprising 255 individuals [30, 31] who met the criteria of being between 20 and 30 years of age (quarter-life age) and consenting to participate in the study, as evidenced by signing an informed consent form. Data were collected using Google Forms, commencing with an explanation of the study, a statement of consent to participate, completion of personal information, and submission of the research scales.
Participants were then required to provide informed consent before proceeding and were given the right to withdraw their consent up to one week after data collection. Complete information regarding the right to withdraw was provided. The contact details of the study team were made available for any inquiries. The procedures were officially approved by the Research Ethics Committee of the Faculty of Medicine, Faculty of Health Sciences, Muhammadiyah University of Surakarta. With ethical eligibility number 598/KEPK-FIK/X/2024.
Participants completed the form in October 2024. To prevent missing data, participants were required to answer all items. The authors also implemented strict quality control measures throughout the sampling procedure to ensure data accuracy. This study utilized “personal data”, a Spiritual Well-being Scale (SWBS), an Emotion Regulation Scale, the Multidimensional Scale of Perceived Social Support (MSPSS), a Short Form Health Survey (SF-36) for Quality of Life, and a Religious Activities Scale. Data from 255 respondents were analyzed. The personal data form provides information on gender, age, and graduate status are shown in Table 1 as follows.
| Profile | Description | Total | Percentage |
|---|---|---|---|
| Gender | Male | 73 | 29% |
| Female | 182 | 71% | |
| Age | 20-23 | 125 | 49% |
| 24-27 | 80 | 31% | |
| 28-30 | 50 | 20% | |
| Graduate | High School | 121 | 47% |
| Associate | 24 | 9% | |
| Bachelor | 103 | 40% | |
| Master | 7 | 3% |
2.2. Quality Of Life Instrument
The Short Form-36 is a standardized general scale used to assess the quality of life and the Cronbach’s alpha coefficient for this scale was 0.789 [32]. Compared to other general instruments, it provides a comprehensive evaluation by encompassing five domains: 1) physical activity limitations due to health problems, 2) social activity limitations due to physical and emotional issues, 3) vitality, 4) daily activity limitations due to emotional issues, and 5) general health perceptions. The SF-36 is expeditious (5-10 minutes), user-friendly, and can be administered via telephone interviews.
Quality of Life (QoL) values were compared with the r-table values. At a significance level of 0.05 and a sample size of 255, the r-table value was 0.1028. In instances where the calculated r-value exceeded that of the r-table, it was considered valid, whereas correlation values lower than the r-table indicated that the question did not measure the intended concept and was deemed invalid. Consequently, invalid responses were excluded from further analyses. The results revealed that questions QOL20, QOL21, QOL23, QOL24, QOL26, QOL27, QOL30, and QOL34 exhibited correlation values lower than the r-table, and were thus eliminated. This resulted in a final set of 28 valid questions for the subsequent analysis.
2.2.1. Quality of Life Reliability Test (QoLRT)
A reliability test is a test that shows the extent to which a measuring instrument is reliable or trustworthy. The reliability test is seen from the Cronbach's Alpha value and fulfilled if the Cronbach's Alpha value is > 0.7. The reliability results for variable Quality of Life is shown in Table 2 as follows.
| - | N | % | |
|---|---|---|---|
| Cases | Valid | 255 | 100.0% |
| Excludeda | 0 | 0% | |
| Total | 255 | 100.0% | |
Table 3 showed a Cronbach's alpha value of 0.734 for 29 items. The questionnaire was considered reliable because its value was greater than 0.70.
| Cronbach's Alpha | No. of Items |
|---|---|
| 0.734 | 29 |
2.3. Spiritual Well-being Instrument
The Spiritual Well-Being Scale (SWBS) and its translations are available without cost for research, teaching, clinical practice, public speaking, or other scholarly endeavors, provided that appropriate citations and acknowledgements are included in any publication or presentation of work conducted using the SWBS with values RMSEA 0.46 and CFI 0.96 for this scale [33].
The Spiritual Well-Being (SWB) values were compared with the r-table values, utilizing a significance level of 0.05, the sample size of 255, and r-table value of 0.1028. Questions with a calculated r-value exceeding the r-table value were deemed valid, whereas those below this value were considered invalid. The analysis revealed that question SWB13 exhibited a correlation value lower than the r-table value and was consequently eliminated, leaving 19 valid questions.
2.3.1. Spiritual Well-being Reliability Test (SWRT)
A reliability test is a test that shows the extent to which a measuring instrument is reliable or trustworthy. The reliability of the test is assessed using Cronbach's Alpha, with a value greater than 0.7 indicating acceptable reliability, as shown in Table 4. The reliability results for variable Spiritual Well-Being are shown in Table 5 as follows
| - | N | % | |
|---|---|---|---|
| Cases | Valid | 255 | 100.0% |
| Excludeda | 0 | 0% | |
| Total | 255 | 100.0% | |
| Cronbach's Alpha | No. of Items |
|---|---|
| 0.765 | 20 |
Reliability analysis yielded a Cronbach's alpha coefficient of 0.765 for the 20 items, as shown in Table 5. The questionnaire was considered reliable as the coefficient exceeded the conventional threshold of 0.70.
2.4. Emotion Regulation Instrument
The Emotion Regulation Questionnaire (ERQ) was originally developed by a study and later adapted by another, with a reported Cronbach’s alpha coefficient of 0.80 for the scale [34, 35]. The ERQ comprises 10 items, with six items measuring the cognitive reappraisal dimension (ERQ-CR) and four items assessing expressive suppression (ERQ-ES). The validity of the ERQ was evaluated using Pearson's item-rest correlation, which yielded a score range of r = 0.213–0.584 for ERQ-CR and r = 0.278–0.517 for ERQ-ES, thus demonstrating reliability based on a threshold of r ≥ 0.20, [36]. Reliability assessment, conducted using Cronbach's alpha method, resulted in reliability coefficients of α = 0.692 for ERQ-CR and α = 0.529 for ERQ-ES, categorizing them as moderately reliable. The emotion regulation scale in this investigation underwent cross-cultural adaptation, following the methodologies outlined by a few studies [37, 38].
Emotion Regulation (ER) values were compared with the r-table values. At a significance level of 0.05 and a sample size of 255, the r-table value was 0.1028. Calculated r-value exceeding the r-table value were considered valid, whereas lower values indicated invalid questions. Questions ER1R and ER4R exhibited correlation values lower than the r-table value and were subsequently removed, leaving eight valid questions.
2.4.1. Emotion Regulation Reliability Test (ERRT)
A reliability test is a test that shows the extent to which a measuring instrument is reliable or trustworthy. The reliability test is seen from the Cronbach's Alpha value and fulfilled if the Cronbach's Alpha value is > 0.7 as shown at Table 6.
The reliability test results in table 7 showed a Cronbach's alpha value of 0.738 for the nine items. The questionnaire was considered reliable because its value was greater than 0.70.
2.5. Social Support Instrument
The Multidimensional Scale of Perceived Social Support (MSPSS) was developed by another study and the Cronbach’s alpha coefficient for this scale was 0.85 [39]. This scale comprises 12 items divided into three subscales: family support (items 3, 4, 8, and 11; α = 0.929), friend support (items 6, 7, 9, and 12; α = 0.942), and significant others (items 1, 2, 5, and 10; α = 0.941). Social Support (SS) values were compared with the r-table values. With a significance level of 0.05 and a sample size of 255, the r-table value was 0.1028. Items with calculated r-values exceeding the r-table were deemed valid, whereas those with lower values indicated invalid responses. Items SS5, SS7, and SS8 exhibited correlation values lower than the r-table and were subsequently removed, resulting in 19 valid items.
| - | N | % | |
|---|---|---|---|
| Cases | Valid | 255 | 100.0% |
| Excludeda | 0 | 0% | |
| Total | 255 | 100.0% | |
| Cronbach's Alpha | No. of Items |
|---|---|
| 0.738 | 9 |
2.5.1. Social Support Reliability Test (SSRT)
A reliability test is a test that shows the extent to which a measuring instrument is reliable or trustworthy. The reliability test is seen from the Cronbach's Alpha value and fulfilled if the Cronbach's Alpha value is > 0.7, as shown in Table 8. The reliability results for variable Social Support are shown in Table 9 as follows.
| - | N | % | |
|---|---|---|---|
| Cases | Valid | 255 | 100.0% |
| Excludeda | 0 | 0% | |
| Total | 255 | 100.0% | |
| Cronbach's Alpha | No. of Items |
|---|---|
| 0.763 | 10 |
The questionnaire was deemed reliable, because its value exceeded 0.70.
2.6. The Religious Activities Instrument
The Religious Activities Scale was adapted from a study and the Cronbach’s alpha coefficient for this scale was 0.612 [40]. This scale comprises two aspects with the following indicators: 1) internal aspects, including motivation, intensity, and attention, and 2) external aspects, including family, school, and peer influence.
Religious activity (RA) values were compared to r-table values. With a significance level of 0.05 and a sample size of 255, the r-table value was 0.1028. Items with calculated r-value that exceeded the r-table were deemed valid, whereas those with lower values were considered invalid. Item RA7 exhibited a correlation value lower than that of the r-table and was subsequently removed, resulting in 17 valid items.
2.6.1. Religious Activities Reliability Test (RART)
A reliability test is a test that shows the extent to which a measuring instrument is reliable or trustworthy. The reliability of the test is assessed using Cronbach's Alpha, with a value greater than 0.7 indicating acceptable reliability, as shown in Table 10. The reliability results for variable Religious Activities are shown in Table 11.
The reliability test results indicated a Cronbach's alpha coefficient of 0.746 for 18 items. A value exceeding 0.70 was considered indicative of questionnaire reliability. The researcher may utilize items that meet the established psychometric criteria. Subsequently, the reliability coefficient was calculated, and the scale was employed owing to its high reliability [41].
| - | N | % | |
|---|---|---|---|
| Cases | Valid | 255 | 100.0% |
| Excludeda | 0 | 0% | |
| Total | 255 | 100.0% | |
| Cronbach's Alpha | No. of Items |
|---|---|
| 0.746 | 18 |
The investigation of Quality of Life proceeded with Structural Equation Model (SEM) analysis to determine the correlations among variables. The initial step involves conducting a normality test, as shown in Table 12
| Variable | Min | Max | Skew | C.R. | Kurtosis | C.R. |
|---|---|---|---|---|---|---|
| QOL36 | 1.000 | 4.000 | 0.352 | 2.296 | -0.834 | -2.719 |
| QOL35 | 1.000 | 4.000 | -3.804 | -24.796 | 14.500 | 47.265 |
| QOL34 | 1.000 | 4.000 | 0.525 | 3.421 | -0.631 | -2.057 |
| QOL33 | 1.000 | 4.000 | -0.886 | -5.778 | -0.432 | -1.408 |
| QOL32 | 1.000 | 4.000 | -0.798 | -5.204 | -0.098 | -0.320 |
| QOL31 | 1.000 | 4.000 | -0.333 | -2.174 | -0.825 | -2.688 |
| QOL30 | 1.000 | 4.000 | 0.014 | 0.093 | -0.842 | -2.745 |
| QOL29 | 1.000 | 4.000 | -0.547 | -3.568 | -0.569 | -1.854 |
| QOL28 | 1.000 | 4.000 | -0.796 | -5.189 | -0.014 | -0.044 |
| QOL27 | 1.000 | 4.000 | -0.230 | -1.500 | -0.740 | -2.412 |
| QOL26 | 1.000 | 4.000 | -0.280 | -1.826 | -0.744 | -2.425 |
| QOL25 | 1.000 | 4.000 | -1.015 | -6.618 | 0.291 | 0.950 |
| QOL24 | 1.000 | 4.000 | 0.891 | 5.808 | -0.465 | -1.515 |
| QOL23 | 1.000 | 4.000 | -0.244 | -1.591 | -0.790 | -2.575 |
| QOL22 | 1.000 | 4.000 | -0.291 | -1.894 | -1.010 | -3.293 |
| QOL21 | 1.000 | 5.000 | 0.486 | 3.168 | -0.660 | -2.150 |
| QOL1 | 1.000 | 4.000 | -0.493 | -3.215 | -0.059 | -0.191 |
| QOL2 | 1.000 | 4.000 | -0.989 | -6.445 | -0.454 | -1.481 |
| QOL20 | 1.000 | 5.000 | 0.478 | 3.118 | -0.699 | -2.280 |
| QO19 | 1.000 | 4.000 | -0.310 | -2.018 | -1.904 | -6.207 |
| QOL18 | 1.000 | 4.000 | -0.484 | -3.158 | -1.758 | -5.731 |
| QOL17 | 1.000 | 4.000 | -0.580 | -3.780 | -1.664 | -5.423 |
| QOL16 | 1.000 | 4.000 | -0.693 | -4.515 | -1.508 | -4.917 |
| QOL15 | 1.000 | 4.000 | -0.989 | -6.445 | -1.023 | -3.333 |
| QOL14 | 1.000 | 4.000 | -0.652 | -4.248 | -1.575 | -5.135 |
| QOL13 | 1.000 | 4.000 | -0.759 | -4.948 | -1.420 | -4.628 |
| QOL12 | 1.000 | 4.000 | -3.189 | -20.790 | 8.750 | 28.523 |
| QOL11 | 1.000 | 4.000 | -1.930 | -12.584 | 2.097 | 6.836 |
| QOL10 | 1.000 | 4.000 | -1.431 | -9.326 | 0.364 | 1.185 |
| QOL9 | 1.000 | 4.000 | -0.819 | -5.338 | -1.038 | -3.383 |
| QOL8 | 1.000 | 4.000 | -1.403 | -9.148 | 0.282 | 0.920 |
| QOL7 | 1.000 | 4.000 | -2.643 | -17.230 | 5.501 | 17.932 |
| QOL6 | 1.000 | 4.000 | -1.638 | -10.678 | 1.028 | 3.352 |
| QOL5 | 1.000 | 4.000 | -2.505 | -16.333 | 4.759 | 15.513 |
| QOL4 | 1.000 | 4.000 | -1.364 | -8.890 | 0.179 | 0.584 |
| QOL3 | 1.000 | 4.000 | 0.153 | 0.998 | -1.550 | -5.053 |
| SWB1 | 1.000 | 4.000 | 0.990 | 6.452 | -0.030 | -0.097 |
| SWB2 | 1.000 | 4.000 | 1.081 | 7.044 | 0.084 | 0.273 |
| SWB20 | 1.000 | 4.000 | 1.618 | 10.548 | 1.868 | 6.090 |
| SWB19 | 1.000 | 4.000 | 1.257 | 8.196 | 0.817 | 2.664 |
| SWB18 | 1.000 | 4.000 | 1.053 | 6.862 | -0.039 | -0.128 |
| SWB17 | 1.000 | 4.000 | 0.885 | 5.768 | -0.164 | -0.536 |
| SWB16 | 1.000 | 4.000 | 0.345 | 2.252 | -0.715 | -2.332 |
| SWB15 | 1.000 | 4.000 | 1.078 | 7.028 | 0.263 | 0.858 |
| SWB14 | 1.000 | 4.000 | 0.448 | 2.921 | -0.760 | -2.476 |
| SWB13 | 1.000 | 4.000 | -0.698 | -4.550 | -0.641 | -2.090 |
| SWB12 | 1.000 | 4.000 | 0.385 | 2.509 | -0.791 | -2.578 |
| SWB11 | 1.000 | 4.000 | 1.715 | 11.179 | 2.084 | 6.793 |
| SWB10 | 1.000 | 4.000 | 0.219 | 1.425 | -0.629 | -2.050 |
| SWB9 | 1.000 | 4.000 | 0.739 | 4.819 | -0.415 | -1.352 |
| SWB8 | 1.000 | 4.000 | 0.268 | 1.749 | -0.491 | -1.599 |
| SWB7 | 1.000 | 4.000 | 0.906 | 5.905 | -0.298 | -0.971 |
| SWB6 | 1.000 | 4.000 | 0.297 | 1.934 | -1.039 | -3.388 |
| SWB5 | 1.000 | 4.000 | 1.396 | 9.101 | 0.872 | 2.841 |
| SWB4 | 1.000 | 4.000 | 1.980 | 12.906 | 3.344 | 10.901 |
| SWB3 | 1.000 | 4.000 | 2.738 | 17.852 | 7.034 | 22.929 |
| SS1 | 1.000 | 4.000 | -0.904 | -5.891 | -0.301 | -0.983 |
| SS2 | 1.000 | 4.000 | -0.668 | -4.352 | -0.468 | -1.526 |
| SS3 | 1.000 | 4.000 | -0.176 | -1.151 | -0.979 | -3.190 |
| SS4 | 1.000 | 4.000 | -0.679 | -4.424 | -0.342 | -1.113 |
| SS5 | 1.000 | 4.000 | 0.419 | 2.732 | -0.484 | -1.577 |
| SS6 | 1.000 | 4.000 | 0.087 | 0.569 | -0.568 | -1.852 |
| SS7 | 1.000 | 4.000 | 0.387 | 2.524 | -0.627 | -2.045 |
| SS8 | 1.000 | 4.000 | 0.291 | 1.897 | -0.639 | -2.082 |
| SS9 | 1.000 | 4.000 | -0.610 | -3.977 | -0.706 | -2.300 |
| SS10 | 1.000 | 4.000 | -0.520 | -3.387 | -0.844 | -2.751 |
| SS11 | 1.000 | 4.000 | -0.552 | -3.601 | -0.792 | -2.582 |
| SS12 | 1.000 | 4.000 | -0.490 | -3.191 | -0.984 | -3.207 |
| ER1 | 1.000 | 4.000 | -0.312 | -2.037 | -0.939 | -3.060 |
| ER2 | 1.000 | 4.000 | 0.576 | 3.758 | -0.608 | -1.981 |
| ER3 | 1.000 | 4.000 | 0.223 | 1.453 | -0.763 | -2.488 |
| ER4 | 1.000 | 4.000 | 0.412 | 2.687 | -0.636 | -2.073 |
| ER5 | 1.000 | 4.000 | 0.771 | 5.028 | -0.593 | -1.934 |
| ER6 | 1.000 | 4.000 | 0.070 | 0.459 | -1.035 | -3.375 |
| ER7 | 1.000 | 4.000 | 0.463 | 3.018 | -0.763 | -2.486 |
| ER8 | 1.000 | 4.000 | 0.309 | 2.017 | -0.674 | -2.196 |
| ER9 | 1.000 | 4.000 | 0.290 | 1.893 | -1.022 | -3.331 |
| ER10 | 1.000 | 4.000 | 0.351 | 2.291 | -0.563 | -1.836 |
| RA1 | 1.000 | 4.000 | 0.958 | 6.243 | -0.135 | -0.440 |
| RA2 | 1.000 | 4.000 | 1.039 | 6.776 | 0.024 | 0.079 |
| RA3 | 1.000 | 4.000 | 0.836 | 5.448 | -0.395 | -1.288 |
| RA4 | 1.000 | 4.000 | 1.244 | 8.107 | 0.596 | 1.942 |
| RA5 | 1.000 | 4.000 | 0.097 | 0.631 | -0.755 | -2.463 |
| RA6 | 1.000 | 4.000 | 0.746 | 4.862 | -0.263 | -0.857 |
| RA7 | 1.000 | 4.000 | -0.431 | -2.808 | -0.840 | -2.737 |
| RA8 | 1.000 | 4.000 | 0.994 | 6.483 | 0.132 | 0.430 |
| RA9 | 1.000 | 4.000 | 1.187 | 7.741 | 0.367 | 1.198 |
| RA10 | 1.000 | 4.000 | -0.028 | -0.182 | -0.640 | -2.086 |
| RA11 | 1.000 | 4.000 | -0.025 | -0.165 | -0.898 | -2.927 |
| RA12 | 1.000 | 4.000 | 0.905 | 5.897 | -0.090 | -0.293 |
| RA13 | 1.000 | 4.000 | 0.768 | 5.010 | -0.418 | -1.361 |
| RA14 | 1.000 | 4.000 | -0.058 | -0.377 | -0.794 | -2.589 |
| RA15 | 1.000 | 4.000 | 0.146 | 0.950 | -0.746 | -2.431 |
| RA16 | 1.000 | 4.000 | 0.044 | 0.285 | -0.959 | -3.125 |
| RA17 | 1.000 | 4.000 | 0.682 | 4.449 | -0.138 | -0.450 |
| RA18 | 1.000 | 4.000 | 1.186 | 7.732 | 0.660 | 2.151 |
| Multivariate | - | - | - | - | 508.400 | 29.593 |
The data used in this study were derived from primary research based on responses from diverse respondents, presenting challenges in obtaining data that precisely adhere to a multivariate normal distribution [42]. The subsequent measurement, Goodness of Fit (GOF), evaluates the congruence between the observational input and the predictions from the proposed model. Analysis of the AMOS results indicates that the five criteria are deemed less satisfactory than the seven criteria. Consequently, modification of the measurement of endogenous variables is warranted. The objective of the modification indices is to obtain values that correspond to the reference values of the structural model equations, as delineated in the modification index in Table 13.
| Error | Indicator |
|---|---|
| e64 | QOL6 |
| e65 | QOL |
| e66 | QOL8 |
| e67 | QOL9 |
| e68 | QOL10 |
| e69 | QOL11 |
| e70 | QOL12 |
| e9 | SS4 |
| e11 | SS2 |
| e30 | RA1 |
| e44 | SWB6 |
| e48 | SWB10 |
| e5 | SS8 |
| e21 | ER2 |
| e6 | SS7 |
| e17 | ER6 |
| e31 | RA10 |
Subsequent to the modification of indices through the elimination of indicators exhibiting the highest errors and those with the most frequent errors, as indicated in the modification indices and presented in the aforementioned table, the resultant changes in the goodness-of-fit statistics mentioned in Table 14.
A study mentions the consensus of the researchers who state that Chi-square is not the only measure of Goodness of Fit (GoF) and there is no GoF size that exclusively represents the overall model fit [43]. The model fit suggests that the suitability of the model developed through empirical data is at least seen from the fulfillment of two of the three different model fit category sizes namely absolute fit measures, incremental fit measures, and parsimonious fit measures. It also refers to opinion, which suggests that the use of Chi-square is sensitive to the size of the sample used [44].
| Goodness of Fit Index | Cut of Value | Analysis result | Model Evaluation |
|---|---|---|---|
| CMIN/DF | <2 or <3 | 2,092 | Fit |
| P | >0.05 | 0,007 | Marginal |
| GFI | >0.90 | 0.960 | Fit |
| RMSEA | <0.08 | 0.066 | Fit |
| AGFI | >0.90 | 0.907 | Fit |
| TLI | >0.95 | 0.977 | Fit |
| CFI | >0.95 | 0.947 | Fit |
The adapted scale shows a good fit for most criteria between the measurement model and the data, where indicators such as GFI, CFI, and RMSEA are within acceptable limits. It is an appropriate approach for assessing model fit in multidimensional measures in psychology [45]. In Structural Equation Modeling (SEM), the chi-square test is commonly used to assess the model fit. However, it is highly sensitive to sample size, often leading to significant p-values in large samples even when the model fits well. This sensitivity can result in the rejection of a well-fitted model based solely on the chi-square test. Therefore, researchers are advised to consider additional fit indices that are less influenced by sample size. Indices such as the Root Mean Square Error of Approximation (RMSEA), Comparative Fit Index (CFI), and Tucker-Lewis Index (TLI) provide a more nuanced evaluation of model fit. For instance, RMSEA values below 0.05 indicate a good fit, while CFI and TLI values above 0.90 are desirable. By incorporating these alternative fit indices alongside the chi-square test, a more comprehensive and reliable assessment of the model fit can be achieved [45].
The constructs’ aspects remained intact despite item removal, and the model’s validity can still be supported through theoretical justification and other fit indices. Item removal should be based on empirical evidence, such as low factor loadings or high modification indices, to ensure that the retained items adequately represent the construct [30]. Furthermore, if the conceptual meaning of the construct remains unchanged and fit indices such as CFI, TLI, and RMSEA indicate a good model fit, the construct can still be considered robust [46].
Validity Test measuring whether the construct (indicator) is able or not to reflect the latent variable. An item is said to be valid if the “Loading Factor” or “Standardized Loading Factor” value is more than 0.5. The loading factor value can be seen in Table 15.
| Variable | Item | SLF | Description |
|---|---|---|---|
| SS | SS1 | 0.502 | Valid |
| SS3 | 0.515 | Valid | |
| SS5 | 0.635 | Valid | |
| SS6 | 0.524 | Valid | |
| SS9 | 0.851 | Valid | |
| SS10 | 0.829 | Valid | |
| SS11 | 0.847 | Valid | |
| SS12 | 0.807 | Valid | |
| ER | ER1 | 0.578 | Valid |
| ER3 | 0.509 | Valid | |
| ER4 | 0.599 | Valid | |
| ER5 | 0.672 | Valid | |
| ER7 | 0.685 | Valid | |
| ER8 | 0.704 | Valid | |
| ER9 | 0.593 | Valid | |
| ER10 | 0.529 | Valid | |
| RA | RA2 | 0.7 | Valid |
| RA3 | 0.749 | Valid | |
| RA4 | 0.778 | Valid | |
| RA5 | 0.569 | Valid | |
| RA6 | 0.707 | Valid | |
| RA7 | 0.554 | Valid | |
| RA8 | 0.619 | Valid | |
| RA9 | 0.74 | Valid | |
| RA11 | 0.535 | Valid | |
| RA12 | 0.753 | Valid | |
| RA13 | 0.811 | Valid | |
| RA14 | 0.648 | Valid | |
| RA15 | 0.582 | Valid | |
| RA16 | 0.598 | Valid | |
| RA17 | 0.739 | Valid | |
| RA18 | 0.727 | Valid | |
| SWB | SWB1 | 0.553 | Valid |
| SWB2 | 0.647 | Valid | |
| SWB3 | 0.669 | Valid | |
| SWB4 | 0.659 | Valid | |
| SWB | SWB5 | 0.571 | Valid |
| SWB7 | 0.759 | Valid | |
| SWB8 | 0.514 | Valid | |
| SWB9 | 0.758 | Valid | |
| SWB11 | 0.814 | Valid | |
| SWB12 | 0.577 | Valid | |
| SWB13 | 0.523 | Valid | |
| SWB14 | 0.601 | Valid | |
| SWB15 | 0.737 | Valid | |
| SWB16 | 0.601 | Valid | |
| SWB17 | 0.751 | Valid | |
| SWB18 | 0.532 | Valid | |
| SWB19 | 0.68 | Valid | |
| SWB20 | 0.682 | Valid | |
| QOL | QOL1 | 0.656 | Valid |
| QOL2 | 0.563 | Valid | |
| QOL3 | 0.753 | Valid | |
| QOL4 | 0.526 | Valid | |
| QOL5 | 0.514 | Valid | |
| QOL13 | 0.663 | Valid | |
| QOL14 | 0.546 | Valid | |
| QOL15 | 0.68 | Valid | |
| QOL16 | 0.637 | Valid | |
| QOL17 | 0.575 | Valid | |
| QOL18 | 0.865 | Valid | |
| QOL19 | 0.857 | Valid | |
| QOL20 | 0.789 | Valid | |
| QOL21 | 0.833 | Valid | |
| QOL22 | 0.872 | Valid | |
| QOL23 | 0.839 | Valid | |
| QOL24 | 0.565 | Valid | |
| QOL25 | 0.655 | Valid | |
| QOL26 | 0.629 | Valid | |
| QOL27 | 0.641 | Valid | |
| QOL28 | 0.7 | Valid | |
| QOL29 | 0.603 | Valid | |
| QOL30 | 0.673 | Valid | |
| QOL31 | 0.532 | Valid | |
| QOL32 | 0.598 | Valid | |
| QOL33 | 0.553 | Valid | |
| QOL34 | 0.698 | Valid | |
| QOL35 | 0.675 | Valid | |
| QOL36 | 0.826 | Valid |
| Dependent | ← Independent | Estimate | S.E. | C.R. | P | Label |
|---|---|---|---|---|---|---|
| SWB | SS | 0.090 | 0.026 | 3.420 | *** | par_75 |
| SWB | ER | -0.136 | 0.081 | -1.665 | 0.096 | par_76 |
| SWB | RA | 0.641 | 0.086 | 7.463 | *** | par_77 |
| QOL | SWB | -0.074 | 0.059 | -1.262 | 0.207 | par_78 |
| QOL | RA | -0.019 | 0.036 | -0.520 | 0.603 | par_79 |
| QOL | SS | 0.028 | 0.021 | 1.342 | 0.180 | par_80 |
| QOL | ER | 0.031 | 0.037 | 0.834 | 0.405 | par_81 |
Based on the table above, it can be seen that the Standardized Loading Factor value of no item is smaller than 0.5 so that it is declared valid and the model evaluation process can be continued.
Following the modifications as shown in Fig. (1), one criterion exhibited a value that approached satisfactory. Nevertheless, this result suggests that the model is acceptable in its entirety. Consequently, it can be concluded that the model demonstrates an adequate fit, and further analysis may be conducted.
3. RESULTS
This research explored that the influence of emotional regulation, social support, and religious activities on quality of life was significant through spiritual well-being. Data were analyzed using AMOS SEM software. The results of the data processing test are presented in Table 16.
Hypothesis testing is seen from the estimate value and p-value. Estimate is a value to indicate the direction of a variable relationship. If the estimate value is positive, then the relationship between the variables is positive. Moreover, if the estimate value is negative, then the relationship between the variables is negative. The p-value is the value used to see the significance. If the p-value <0.05, it means that the relationship between variables is significant, whereas a p-value > 0,05, indicates that the relationship between variables is not significant. Table 17 shows the analysis of the hypothesis test results.
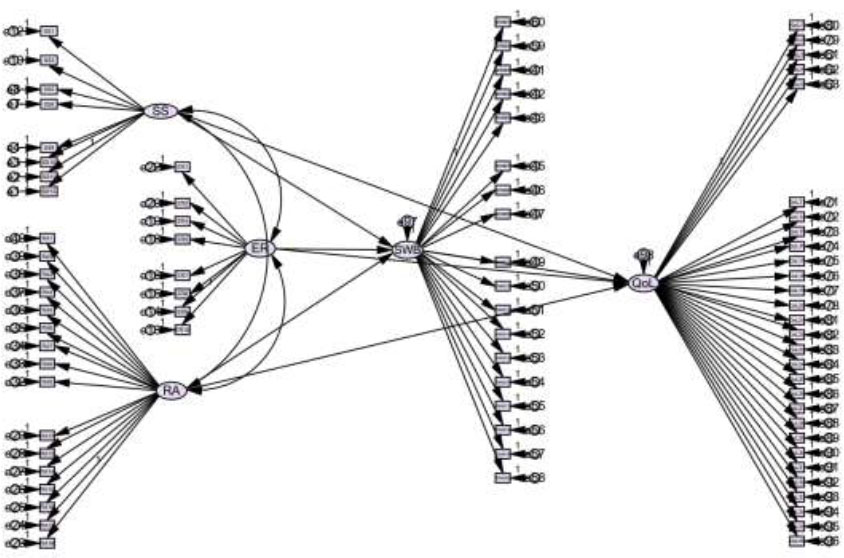
AMOS structural model.
| Estimations | P | Standard Limit | Coefficients |
|---|---|---|---|
| SS → SWB | 0.000 | <0.05 | 0.090 |
| ER → SWB | 0.096 | <0.05 | -1.136 |
| RA → SWB | 0.000 | <0.05 | 0.641 |
| SWB → QOL | 0.207 | <0.05 | -0.74 |
| RA → QOL | 0.603 | <0.05 | -0.019 |
| SS → QOL | 0.180 | <0.05 | 0.028 |
| ER → QOL | 0.405 | <0.05 | 0.031 |
Table 17 representing, if p-value is less than 0.05, it implies a significant relationship between the two things being estimated. If the coefficient is positive, then participation in both estimates will be higher, and vice versa if the p-value is greater than 0.05 or has a negative coefficient.
3.1. Spiritual Well-being (SWB) as a Mediator
This study aimed to determine whether spiritual well-being is a mediator between emotional regulation, social support, and religious activities on quality of life. The mediation test provides the Standardized Direct Effects and Standardized Indirect Effects values. The following equation was used to investigate how ER, SS, and RA affect QOL, with SWB serving as a mediating factor.
Table 18 presents a comparison of standardized direct and indirect effect values to determine whether SWB functions as an intervening variable in the relationships between RE, SS, RA, and QOL. This analysis suggests that when the standardized direct effects are less than the standardized indirect effects, it can be concluded that the mediating variable exerts an indirect influence on the relationship between the independent and dependent variables. Direct effects are weaker because spiritual well-being advances knowledge of emotion regulation, social support, and religious activities during the quarter-life crisis.
| - | Standardized Direct Effects | Standardized Indirect Effects |
|---|---|---|
| RA | -0.088 | 0.224 |
| ER | 0.021 | 0.040 |
| SS | 0.008 | 0.049 |
The data presented in the table indicate that the normalized direct effects of RA, ER, and SS on QOL are less substantial than their indirect effects. This implies a notable indirect connection between RA, ER, and SS in relation to QOL. Such findings point to Spiritual Well-Being (SWB) as a mediator in this relationship. The outcomes are summarized as follows:
1. There is a significant relationship between social support and quality of life through spiritual well-being.
2. There was a significant relationship between emotion regulation and quality of life through spiritual well-being.
3. There was a significant relationship between religious activities and quality of life through spiritual well-being.
The analysis of standardized indirect effects offers important insights into the mediating role of Spiritual Well-Being (SWB) in the relationship between quarter-life crisis experiences and Quality of Life (QoL). The standardized indirect effect exceeded the standardized direct effect, which shows the mediating influence of SWB. This pattern indicates that, although SWB may technically meet the statistical criteria for mediation, its practical significance in influencing the quality of life outcomes during quarter-life crises may be limited. A mediating variable transmits the effect of an independent variable on a dependent variable, often resulting in an indirect effect that can be larger than a direct effect. This occurs when the mediator partially explains the relationship between independent and dependent variables, highlighting the importance of considering indirect pathways in research [47, 48]
Social support, emotion regulation, and religious activities are expected to have an increasing influence on spiritual well-being. Spiritual Well-Being interventions serve as a powerful catalysts for comprehensive quality-of-life improvements across multiple domains, functioning as transformative mediators that amplify the traditional healthcare approaches while addressing deeper existential needs. Religious/spiritual coping could also be a significant factor in promoting the psychological functioning of university students [49, 50].
4. DISCUSSION
The present research explored the influence of social support, emotion regulation, and religious activities based on spiritual well-being. Individuals who can maintain their spiritual well-being are able to enhance their quality of life by managing their emotions, developing quality social relationships and engaging in religious activities [51]. The results reveal that individuals must develop reflective habits and spiritual awareness to better meet challenges that are generally encountered at the quarter-life stage.
4.1. The Impact of Social Support on Quality of Life Through Spiritual Well-being
Spiritual well-being is the sense of tranquility, purpose, and unity that individuals experience in connection with higher principles, whether in secular or religious contexts. Social support within religious communities can significantly influence the deepening of one's comprehension of spiritual values and beliefs. Furthermore, participation in spiritual practices or communal religious events can contribute to the development of stronger social networks that enhance the quality of life [52].
Brief interventions in a positive environment can enhance favorable emotions and decrease anxiety experiencing life difficulties [53]. A study argued that psychological and social elements, including religious convictions and associations, are linked to various social behaviors that enhance the quality of life [54]. In different types of relationships, spirituality within social connections influences mental well-being and quality [55, 56].
4.2. Emotional Regulation's Impact on Life Quality through Spiritual Well-being
Individuals who effectively manage their emotions are better equipped to handle stressful situations without experiencing undue strain. Those adept at emotional regulation tend to have lower anxiety levels and a more favorable stress response, which ultimately enhances their mental health and overall quality of life [34]. The ability to control negative emotions such as anger or anxiety leads to improved emotional well-being. This contributes to greater life satisfaction, thankfulness, and a positive life perspective, supported by spiritual well-being, which is a crucial component of a good quality of life [57, 58].
For young adults, proficient emotional regulation and adaptive emotion management foster positive emotions and the capacity to save the present moment, enhance spiritual well-being, and improve individual quality of life [53, 59, 60]. Robust personal qualities stem from effective emotional regulation, which provides a sense of security and purpose in life. Adaptive emotion regulation is positively associated with cognitive empathy, affective empathy, and compassion and negatively linked to empathic distress [61].
Furthermore, emotional regulation is crucial in cultivating an attitude of gratitude and acceptance, which in turn boosts spiritual well-being. These attitudes help to generate feelings of positivity and meaning in life, which are essential for overall well-being. Interventions that focus on emotional regulation and spiritual practices can yield significant benefits in various contexts [62].
4.3. The Impact of Spiritual Practices on Life Quality through Spiritual Well-being
A strong connection exists between participation in religious activities and enhanced quality of life, with spiritual well-being acting as a mediator. Studies indicate that people who participate in religious practices often experience higher levels of spiritual well-being, which subsequently leads to improved quality of life. Religious engagement has been shown to positively impact commitment to quality in both productive and challenging circumstances [63, 64]. Involvement in religious activities is associated with better quality of life. These practices provide individuals with community support, emotional stability, and an optimistic perspective. Social support derived from religious communities is considered crucial in alleviating the symptoms of depression and anxiety across different age groups and serves as a primary coping strategy [52, 65].
A clear interrelation exists between religion/spirituality and a sense of coherence, with various religious/spiritual approaches leading to a robust sense of coherence [66]. Those with higher religious dedication exhibited the strongest prosocial emotional tendencies (gratitude and awe), and reported seeking meaning in life [67]. This further demonstrates that engaging in religious activities and connecting with spiritual beliefs or faith can significantly enhance emotional well-being and QoL. Spiritual practices and faith can assist individuals in confronting life challenges, boosting mental and cognitive health, and providing a sense of tranquility and satisfaction. Religious involvement contributes to a better quality of life through social support networks, enhanced mental and physical health, and a more positive life outlook.
Religious convictions often emphasize the importance of gratitude, optimism, and hope. Individuals who actively participate in religious activities are more likely to maintain a positive and optimistic perspective on life, enabling them to manage their lives better and positively influence their quality of life [68]. Spiritual well-being enhances the quality of life by influencing an individual's ability to interpret life opportunities, interact with their surroundings, and achieve harmony. A profound understanding of oneself, society, the environment, and the creator is an aspect of spiritual well-being that contributes to improved quality of life. The significance of QOL in this research lies in how it reflects an individual's perception of their life within the context of existing culture and value systems in relation to their goals, expectations, standards, and concerns [69].
4.4. The Role of Spiritual Well-being in Mediating Life Quality During the Quarter-life Period
Spiritual well-being plays a crucial role in emotion regulation, especially during difficult life transitions like the quarter-life crisis. Engaging in spiritual practices allows individuals to gain perspective on their problems, promoting acceptance and emotional growth [70]. This is particularly important for young adults experiencing a quarter-life crisis, as it helps them cope with anxiety and pessimism.
Spiritual well-being also contributes to social support, which is vital during the quarter-life crisis. Spiritual communities often provide a network of support that can buffer stress and enhance well-being [71]. This support is not only emotional but also instrumental, as it encourages healthy lifestyles and discourages harmful behaviors. This suggests that spiritual well-being can enhance the quality of social support, which is crucial for a quarter-life crisis [72]. During the quarter-life crisis, spiritual well-being can serve as a coping mechanism, helping individuals to navigate this challenging phase. Studies have shown that spirituality is one of the most powerful internal influences on the quarter-life crisis, alongside commitment to purpose and anxiety [73].
The significance of QOL among participants in this research serves as a crucial indicator during the Quarter Life phase, a period marked by intense personal and academic growth. Evaluating the quality of life at this stage is essential for gauging overall well-being and accomplishments [74]. To comprehend the relevance of QOL in addressing adult issues, a qualitative approach utilizing a hermeneutic phenomenological design is needed [75].
There is a positive correlation between spiritual well-being and quality of life. Individuals exhibiting higher levels of spiritual well-being tend to experience fewer depressive symptoms and enhanced mental health. Moreover, aspects of spirituality, including purpose and inner peace, positively influence quality of life [76]. The connection between spiritual well-being and quality of life has been established, with spirituality linked to an improved quality of life. Spirituality shapes how people perceive and cope with challenges, subsequently enhancing their QoL [77]. Engaging in spiritual practices, such as prayer and worship, can alleviate anxiety and stress, thereby boosting quality of life.
Various studies have employed the Spiritual Well-Being Scale (SWBS) to evaluate spiritual well-being, which is a crucial component of quality of life. The relationship between spiritual well-being and moral disengagement was examined across age groups. A study indicates that spiritual well-being plays a significant role in comprehending ethical conduct and moral reasoning, which can extend to broader domains. Another study found that psychological factors such as intelligence, personality, and locus of control are linked to religious or spiritual beliefs and behaviors, although this connection varies among generations and types of religious affiliations [54, 78]. religious or Spiritual Well-Being (RSWB) is a key element of subjective well-being and mental health, with potential applications in clinical settings [79].
Spiritual well-being encompasses life purposes, inner tranquility, and connections to higher principles. Engaging in religious practices such as prayer, meditation, and religious ceremonies can enhance spiritual well-being. A study found that a growing Islamic-based spiritual orientation and its elements are linked to improved work-life quality among Muslims [80].
Religious activities often provide social support, with involvement in religious communities offering social networks that foster feelings of acceptance. This social support can alleviate loneliness and boost mental health, positively impacting the quality of life [81]. Religious activities bolstered by social support contribute to spiritual well-being and can serve as coping mechanisms for challenges, offer hope, and enhance one's ability to perceive and comprehend personal experiences and relationships with others and the environment [82]. However, quality of life remains subjective, and a study emphasized the importance of gathering valid and relevant data from individuals living in specific areas for accurate assessment [83].
Spirituality plays a crucial role in promoting well-being during quarter-life crisis. This serves as a coping mechanism and contributes to the overall welfare. Given the strong religious foundation of Indonesian culture, spirituality offers individuals a sense of security and social support, thereby enhancing QoL. Understanding quality of life requires examining individuals' subjective assessments of their well-being in their cultural environment. Various sociodemographic factors can affect a person's overall well-being, thereby influencing their quality of life [84]. In the context of Indonesian society, which is characterized by a religious orientation, further investigation is necessary to determine the Quality of Life and evaluate the extent to which spiritual well-being serves as a mediating variable.
CONCLUSION
The ability to address daily challenges, particularly as one age, is contingent upon an individual's Quality of Life. This research emphasizes the role of spiritual well-being as a mediating factor in attaining Quality of Life, as it offers substantial support to those who already benefit from social connections, emotional management skills, and engagement in religious practices. It not only functions as an intrinsic source of support but also strengthens the benefits derived from various external aspects, such as positive social relationships, emotion regulation skills, and engagement in religious practices. The findings of this study indicate that the internalization of spiritual well-being significantly contributes to enhancing Quality of Life. In other words, individuals who deeply cultivate spiritual well-being are better equipped to handle life pressures, find meaning in their daily experiences, and maintain emotional and psychological balance.
Furthermore, this study highlights the importance of social support and active involvement in religious or spiritual communities as factors that reinforce their internalization process of spiritual well-being. Individuals with strong social networks and access to environments that nurture spiritual growth are more likely to experience the benefits of spiritual well-being in their daily lives. Thus, this research emphasizes that achieving an optimal Quality of Life in not solely determined by external factors, such as social and economics conditions, but is also profoundly influenced by internal factors, particularly Spiritual Well-Being. Therefore, efforts to improve Quality of Life should consider strategies that strengthen individuals’ spiritual aspects, whether through education, psychological interventions, or community support oriented toward spiritual and religious values.
STUDY LIMITATION
These findings have important practical implications, indicating that while spiritual well-being may contribute to the relationship between quarter-life crises and quality of life, it should not be considered a primary mechanism of influence. Practitioners should consider these results as evidence for the need to develop more comprehensive intervention strategies that address multiple aspects of young adults' experiences during quarter-life crises. The mediating effects also highlight the importances of identifying and investigating other potential mediating factors that might have a stronger influence on QoL outcomes during this period.
AUTHORS’ CONTRIBUTIONS
It is hereby acknowledged that all authors have accepted responsibility for the manuscript's content and consented to its submission. They have meticulously reviewed all results and unanimously approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| QoL | = Quality of Life |
| I-NAMHS | = Indonesian National Adolescent Mental Health Survey |
| SWBS | = Spiritual Well-being Scale |
| MSPSS | = Multidimensional Scale of Perceived Social Support |
| QoLRT | = Quality of Life Reliability Test |
| SWB | = The Spiritual Well-Being |
| SWRT | = Spiritual Well-Being Reliability Test |
| ERQ | = Emotion Regulation Questionnaire |
| ERQ-CR | = Emotion Regulation Questionnaire-Cognitive Reappraisal |
| ERQ-ES | = Emotion Regulation Questionnaire-Expressive Suppression |
| ER | = Emotion Regulation |
| ERRT | = Emotion Regulation Reliability Test |
| SSRT | = Social Support Reliability Test |
| RA | = Religious Activity |
| RART | = Religious Activities Reliability Test |
| SEM | = Structural Equation Model |
| SF-36 | = Short Form Health Survey: A 36-item questionnaire to measure overall health status and quality of life. |
| GOF | = Goodness of Fit |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Research Ethics Committee of the Faculty of Medicine, Faculty of Health Sciences, Muhammadiyah University of Surakarta, Indonesia with ethical eligibility number 598/KEPK-FIK/X/2024.
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from all participants prior to their involvement in the study. Consent was collected through a Google Form, in which participants were clearly informed about the purpose of the research, and their voluntary participation was explicitly requested without any coercion.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available in the Open Science Framework at the following link: https://osf.io/gj6pv/?view_only=1aad249646894adfbcb148c3e674a4d7.
FUNDING
This research was funded by the Ministry of Education and Culture of Indonesia through the Doctoral Dissertation Research Grant (PDD-DRTPM) in 2024, under contract number 108/E5/PG.02.00.PL/2024. The grant was administered in collaboration with the Faculty of Psychology, Universitas Muhammadiyah Surakarta, Indonesia.
ACKNOWLEDGEMENTS
The authors gratefully acknowledge the Ministry of Education, Culture, Research, and Technology of the Republic of Indonesia for their generous financial support that made this research possible. Moreover, appreciation is extended to young adults aged 20–30 years in Surakarta who willingly participated in the study.

