All published articles of this journal are available on ScienceDirect.

A Systematic Review of Mindfulness-based Stress Reduction (MBSR) and Its Effects on Mental Health and Academic Performance in University Students
Abstract
Introduction
Mindfulness-Based Stress Reduction (MBSR) is increasingly recognized for its role in improving university students' mental health and academic performance. This systematic review evaluates the impact of MBSR on stress, anxiety, depression, cognitive flexibility, and emotional regulation.
Methods
Following PRISMA guidelines, 34 high-quality studies published between 2012 and 2024 were analyzed, covering student populations in healthcare, psychology, business, and technical fields.
Results
Findings indicate that MBSR significantly reduces perceived stress (up to 33%) and mental health issues (by 40%), particularly in academic settings and low- to middle-income countries. Traditional in-person MBSR interventions significantly reduce stress, anxiety, and depression while improving cognitive flexibility and emotional regulation. Digital MBSR programs offer comparable psychological benefits but face engagement challenges. Discipline-specific variations revealed that healthcare and psychology students experience the most significant improvements, business students enhance decision-making skills, and STEM students show cognitive flexibility gains but lower participation rates. RCTs confirm a causal relationship between MBSR and mental health improvements, while observational studies highlight its real-world applicability despite higher dropout rates.
Discussion
Theoretical models, including Cognitive Load Theory (CLT), Self-Regulation Theory (SRT), and Mindfulness-Based Cognitive Therapy (MBCT), provide a foundation for understanding MBSR's impact on cognitive processing, self-regulation, and emotional resilience. Despite promising results, small sample sizes, short intervention durations, and variability in study designs limit generalizability. Future research should refine digital adaptations, implement hybrid mindfulness models, and address discipline-specific needs.
Conclusion
In conclusion, MBSR emerges as a valuable intervention for fostering students’ mental health and academic success.
1. INTRODUCTION
The Mindfulness-Based Stress Reduction (MBSR) intervention, initially developed for stress management, is now being employed to treat a range of conditions, including depression, anxiety, chronic pain, cancer, diabetes mellitus, hypertension, as well as skin and immunological problems [1]. Furthermore, mindfulness-based interventions have been shown to help improve mental health in patients with physical health conditions as well [2]. For those with chronic pain, for example, mindfulness can normalize psychology and nerves and increase internal and external connectivity to networks of work related to stress perception, cognition, and emotion [3]. Preliminary evidence from other studies suggests that practicing mindfulness can strengthen immunity, regulate inflammation, and aging of immune cells [4].
More than 720 hospitals and clinics worldwide offer MBSR as an alternative treatment option to patients [5]. It consists of 2.5 hours/week, 8-week sessions with 1-and-a-half-day meditation retreats [6]. Participants receive instructions on formal mindfulness meditation techniques, including body scanning, mental and emotional awareness, breathing exercises, walking and sitting meditation, and stress management [7]. Participants are also involved in daily home practice tasks (formal) and are encouraged to integrate mindfulness into their daily activities (informal) [8]. Research has shown that MBSR can significantly reduce symptoms of anxiety, depression, and chronic pain, improving overall well-being and quality of life [9-11]. In recent years, there has been an increased interest in the application of mindfulness and stress reduction practices in educational settings to enhance students' mental health and positive outcomes. University students are certainly familiar with their vulnerability to stress, especially due to academic stress, and it is closely related to psychological well-being [12]. In addition to its clinical applications, MBSR has been shown to significantly improve psychological well-being and academic performance among university students by reducing stress, increasing self-efficacy, and promoting mindfulness [13-15]. For instance, a review of 209 studies was conducted on mindfulness experiments, including 12,145 individuals, and discovered that mindfulness-based therapy was especially effective at lowering stress, anxiety, and depression [16].
Several studies have used an evidence-based medical approach to examine the effects of MBSR treatment on reducing psychological distress, improving psychological well-being, reducing stress and anxiety levels, and improving overall well-being and mental health of university students [17-21]. This systematic review evaluates the impact of MBSR on university students' mental health and academic performance. It assesses its effects on reducing depression, anxiety, stress, emotional regulation, cognitive flexibility, academic performance, and the efficacy of digital and app-based mindfulness interventions.
2. MATERIALS AND METHODS
2.1. Inclusion and Exclusion Criteria
This systematic review evaluates the effects of MBSR on the psychological well-being and academic performance of university students. To provide a broader contextual understanding, the review also considers studies on related Mindfulness-Based Therapies (MBTs) that share conceptual and methodological similarities with MBSR. These include Mindfulness-Based Cognitive Therapy (MBCT), Dispositional Mindfulness, Acceptance and Commitment Therapy (ACT), Mindfulness Meditation Training Program (MMTP), Mindfulness-Based Interventions (MBIs), and Mindfulness-Based Student Training (MBST). While the primary focus remains on MBSR, incorporating these related interventions allows for a more comprehensive synthesis of findings regarding mindfulness-based approaches in academic settings.
This review includes quantitative studies published in English between 2012 and 2024, ensuring that the findings reflect recent developments in mindfulness research and its application in higher education. The databases selected (PubMed, ScienceDirect, and PsycINFO) were chosen due to their high indexing standards, relevance to psychological and health-related disciplines, and broad coverage of peer-reviewed empirical studies on mindfulness interventions. These databases ensured the inclusion of rigorously vetted, high-quality sources aligned with the review's quantitative focus and PRISMA guidelines. Grey literature, including theses, dissertations, and unpublished reports, was excluded to maintain methodological consistency and ensure that only peer-reviewed studies with standardized reporting protocols were analyzed. However, the exclusion of grey literature may have led to publication bias and the omission of potentially valuable insights, especially from non-traditional or emerging intervention formats. This limitation is acknowledged, suggesting the need for future reviews to consider a broader inclusion of literature for a more comprehensive understanding.
To maintain a focused scope, only studies that specifically examine university and college student populations were considered. The selected studies evaluated MBSR’s impact on stress, anxiety, depression, emotional regulation, cognitive flexibility, and academic performance. Exclusion criteria were established to ensure methodological rigor and relevance. The review excluded the following (Table 1):
| Exclusion Category | Reason for Exclusion |
|---|---|
| Qualitative studies, review articles, case studies, and editorials | These sources do not provide statistical analyses suitable for quantitative synthesis. |
| Studies focusing solely on clinical populations (e.g., individuals diagnosed with psychiatric disorders) | The psychological profiles of clinical populations differ from the general student population, limiting generalizability. |
| Studies on children, adolescents, or non-university adult populations | To maintain consistency, the review focuses solely on university students. |
| Research lacking sufficient psychological outcome data | Studies that do not measure stress, anxiety, depression, or cognitive outcomes in relation to MBSR interventions were excluded. |
2.2. Data Sources and Search Strategy
This systematic review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to ensure a transparent, comprehensive, and replicable search strategy. A structured literature search was conducted across three major academic databases: PubMed, ScienceDirect, and PsycINFO, selected for their extensive coverage of peer-reviewed research in psychology, medicine, and education.
To optimize search precision and maximize relevant study retrieval, Boolean operators (AND, OR) and database-specific search strings were applied. Search terms were selected based on key concepts related to MBSR and its psychological and academic outcomes among university students. The primary search strategy incorporated a combination of the following keywords:
1. Intervention terms: “Mindfulness-Based Stress Reduction (MBSR),” “Mindfulness-Based Interventions (MBIs),” “Mindfulness-Based Cognitive Therapy (MBCT),” “Mindfulness Meditation Training Program (MMTP).”
2. Outcome-related terms: “psychological well-being,” “mental health,” “stress reduction,” “anxiety,” “depression,” “emotional regulation,” “cognitive flexibility.”
3. Population-related terms: “university students,” “college students,” “higher education.”
Search queries were adapted for each database to ensure compatibility with database-specific indexing systems and search algorithms. The search process included both title, abstract, and keyword-based searches to capture relevant literature comprehensively. Reference lists of key studies were also manually screened to identify additional eligible studies that may not have appeared in the initial search results.
To ensure the reliability and validity of the search strategy, two independent reviewers screened retrieved articles by assessing titles and abstracts based on predefined inclusion criteria. Full-text reviews were conducted for studies meeting the initial selection criteria, and discrepancies in study inclusion were resolved through discussion. Grey literature, unpublished dissertations, and conference proceedings were excluded to maintain methodological rigor and limit potential publication bias.
2.3. Study Selection and Screening
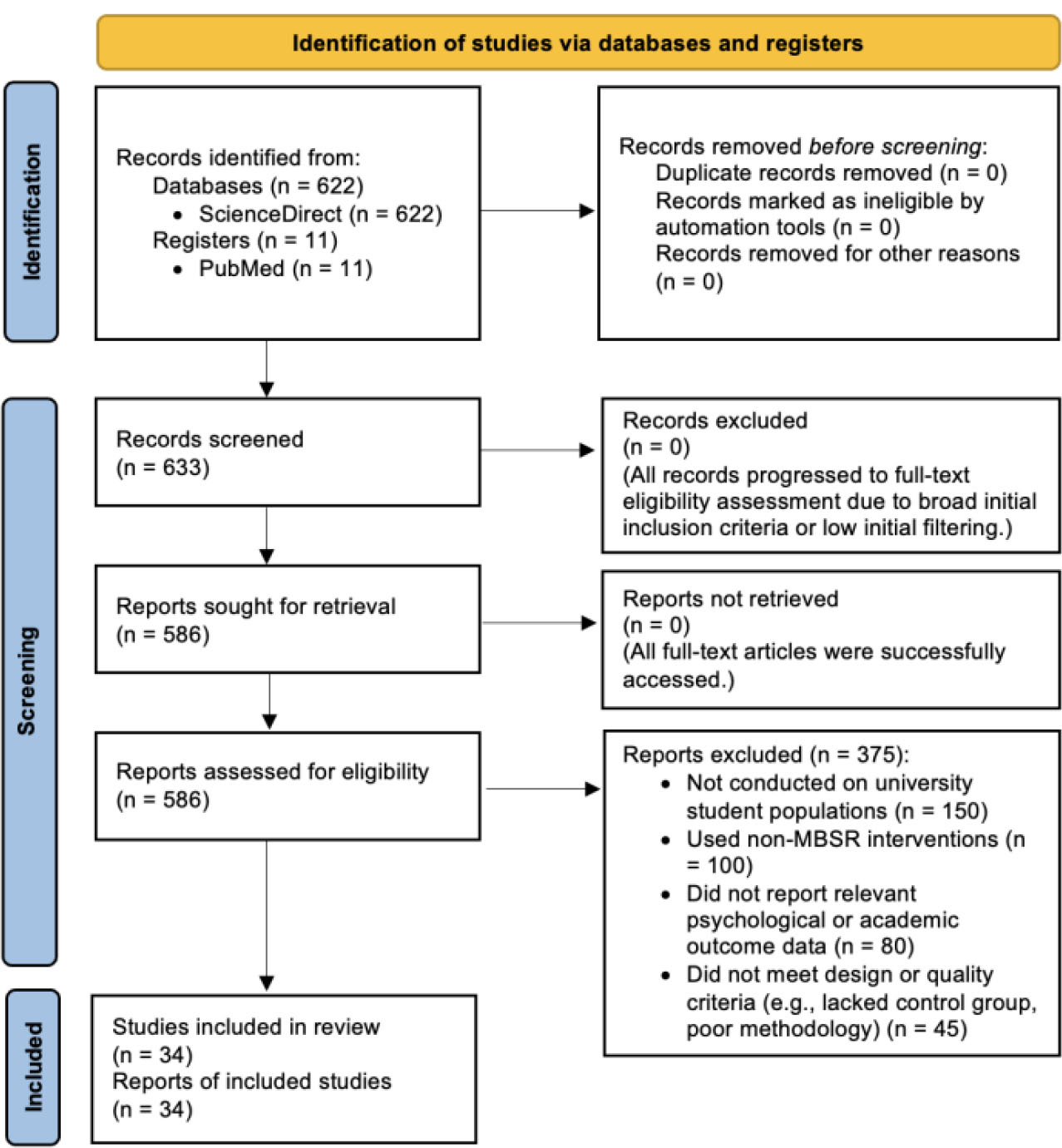
The initial search yielded a total of 633 records, with 622 articles retrieved from ScienceDirect and an additional 11 from PubMed. No additional studies were obtained from PsycINFO due to database restrictions. These records were imported into a reference management system, where duplicate entries were automatically identified and removed before proceeding with the screening process.
The first stage of screening involved an independent review of article titles and abstracts to eliminate studies that did not meet the predefined inclusion criteria. At this stage, 620 records were excluded for various reasons, including studies that did not focus on university or college students, research that did not involve MBSR interventions, articles that lacked psychological or academic outcome measures, and studies that were review articles, commentaries, or case studies rather than empirical research. Following this initial screening, 586 articles proceeded to full-text assessment to determine their eligibility for inclusion in the final synthesis. During the full-text review stage, an additional 375 studies were excluded. Specifically:
1. 150 studies did not focus on university students as the target population,
2. 100 studies explored mindfulness-related interventions but did not implement MBSR as the primary intervention,
3. 80 studies lacked sufficient outcome data related to psychological well-being or academic performance,
4. 45 studies did not meet study design criteria, as they were review papers, qualitative studies, or case reports.
After applying these exclusion criteria, a final total of 34 studies were selected for inclusion in the qualitative and quantitative synthesis. These studies represented a diverse range of research methodologies, including randomized controlled trials (RCTs), quasi-experimental studies, and observational designs, ensuring a comprehensive evaluation of MBSR’s effects on university students. A PRISMA flow diagram (Fig. 1) visually illustrates this step-by-step refinement process.
2.4. Data Extraction and Quality Assessment
Data extraction was conducted independently by two reviewers using a standardized extraction form to ensure consistency and accuracy (Table 2). The extracted variables included study design, sample size, intervention type, duration, outcomes measured, and statistical results. This structured approach facilitated a comprehensive analysis of MBSR interventions and their effects on university students.
| Variable | Details Extracted |
|---|---|
| Study Characteristics | Author(s), year, country, study design, sample size |
| Participant Characteristics | Age, gender, academic discipline, baseline mental health status |
| Intervention Details | Type (in-person, online, app-based), duration, frequency, facilitator. |
| Outcome Measures | Stress, anxiety, depression, emotional regulation, cognitive flexibility, and academic performance. |
| Assessment Tools | DASS-21, PSS, GAD-7, PHQ-9, CFI |
| Statistical Outcomes | Effect sizes, significance levels, and confidence intervals. |
| Risk of Bias | Selection bias, attrition, missing data, study design quality. |
PRISMA flow diagram.
The quality assessment process emphasized methodological rigor, internal validity, and relevance, addressing potential biases in selection, performance, detection, and attrition. Studies exhibiting substantial bias across multiple domains, such as unclear participant selection criteria or inadequate handling of missing data, were excluded to maintain the credibility of the findings. Any discrepancies in the quality assessment were resolved through consensus discussions, ensuring a reliable and unbiased evaluation of the selected studies.
Key psychological well-being outcomes were prioritized during data extraction. These included stress, anxiety, depression, emotional regulation, cognitive flexibility, and overall psychological health. Standardized psychological assessment tools were used to measure these outcomes across studies, with stress, anxiety, and depression commonly assessed using the Perceived Stress Scale (PSS), Generalized Anxiety Disorder-7 (GAD-7), and Patient Health Questionnaire-9 (PHQ-9), respectively. Emotional regulation and cognitive flexibility were evaluated using the Difficulties in Emotion Regulation Scale (DERS) and Cognitive Flexibility Inventory (CFI). Overall psychological health was assessed through validated mental health inventories, ensuring a systematic examination of MBSR’s impact across multiple psychological dimensions.
In addition to psychological outcomes, participant characteristics such as age, gender, field of study, and baseline psychological health status were extracted to enable subgroup analyses. Intervention details, including type, duration, frequency, and delivery mode (in-person or digital adaptations), were also recorded. Study design and funding sources were noted to assess potential conflicts of interest or funding-related biases. In cases where data were missing or unclear, researchers contacted study authors for clarification. If no response was received, conservative estimates were applied to maintain data consistency and reduce reporting bias.
The risk of bias was assessed independently by two reviewers using predefined quality assessment criteria. This process involved a manual evaluation to ensure precision, without the use of automation tools. The assessment focused on selection bias, performance bias, detection bias, and attrition bias. Differences in bias assessments were resolved through discussions, ensuring a rigorous and transparent review process.
This review primarily adopted a qualitative synthesis approach, as statistical pooling was not feasible due to heterogeneity in study designs and outcome measures. Rather than using specific effect measures such as mean differences or risk ratios, findings were presented descriptively, synthesizing reported outcomes across studies. This methodological choice enabled a comprehensive narrative synthesis, capturing broader trends in MBSR effectiveness while acknowledging variations in study design and implementation.
2.5. Data Synthesis and Analysis
This systematic review employed a qualitative synthesis to evaluate the impact of MBSR interventions on the psychological well-being and academic performance of university students. Key outcomes and trends were identified, focusing on variability in intervention duration, sample characteristics (e.g., gender, sample size, baseline psychological health), and reported psychological and academic effects. The findings consistently indicated that MBSR reduced stress, anxiety, and depression, while enhancing emotional regulation, cognitive flexibility, and overall mental health.
This review encompassed 34 high-quality studies with diverse student populations:
1. 10 studies on general university students.
2. 11 studies on healthcare students.
3. 2 studies on psychology students.
4. 1 study each on business, technical college, and international students.
5. 2 studies on female university student-athletes.
6. 1 study each on students with PTSD and eating disorders.
7. 3 studies on students experiencing depression.
8. 1 study on university students in Low- and Middle-Income Countries (LMICs), highlighting the global relevance of MBSR.
Studies were grouped by intervention type (in-person vs. digital adaptations) and target population (e.g., general students vs. students with specific psychological conditions). Missing summary statistics were addressed by contacting the authors. If data remained unavailable, conservative estimates were applied, or the study was excluded if it was deemed insufficient for meaningful synthesis.
Due to heterogeneity in study designs and outcome measures, a narrative synthesis approach was used instead of a meta-analysis. This allowed for a comprehensive qualitative interpretation of variations in study methodologies, participant demographics, and intervention durations.
The risk of bias was assessed by evaluating the completeness of reported outcomes. Studies with significant missing data or selective reporting were deemed to have higher bias risk, affecting the reliability of findings. The certainty of evidence was determined by study design quality and consistency of reported effects. Research with methodological limitations contributed to lower confidence in the results, emphasizing the need for more standardized and rigorous MBSR studies in university settings.
3. RESULTS
3.1. Intervention Type
3.1.1. Traditional (In-Person) Interventions
Traditional MBSR programs, conducted in person, have been widely implemented in university settings to promote mental well-being and stress management. These interventions typically follow an 8-week structured format, incorporating weekly mindfulness training sessions, meditation exercises, body scanning, and stress reduction techniques. Research consistently demonstrates that traditional MBSR interventions lead to significant reductions in stress, anxiety, and depression while fostering improvements in academic performance and emotional regulation. For instance, studies on nursing students [19, 22] and medical students [23] reported improved psychological well-being, emotional regulation, and resilience, particularly in high-stress environments such as clinical training. Additionally, business students exhibited enhanced decision-making abilities, self-efficacy, and reduced stress, demonstrating the cognitive and emotional benefits of mindfulness training [24]. However, engagement levels varied by discipline. While STEM students showed notable improvements in cognitive flexibility and attentional control, they had lower participation rates than humanities students, possibly due to rigid academic schedules and a preference for structured, logic-based learning approaches [25].
Beyond traditional MBSR programs, various mindfulness-based interventions have been tailored to different student groups, demonstrating significant mental health benefits. An 8-week MBSR program for 99 university students and staff led to enhanced mental health, well-being, and nature connectedness [18]. Similarly, among 41 college students in lower-middle-income countries (LMICs), participation in an MBSR program resulted in reduced stress and improved brain activity [17]. Likewise, Brazilian university students who completed the same intervention reported significant stress reduction and an improved quality of life [21].
In addition to MBSR, general mindfulness-based approaches have been integrated into academic settings, producing positive outcomes across diverse student populations. Among Australian and Italian nursing students, mindfulness training, regardless of duration, contributed to notable reductions in stress and psychological distress, with resilience, self-efficacy, and social support acting as key influencing factors [26, 27]. Similarly, multi-modal mindfulness programs for healthcare students resulted in decreased levels of stress, anxiety, and depression while enhancing resilience and well-being [28]. In the U.S., brief mindfulness meditation sessions for university students were effective in improving stress coping mechanisms during social evaluative stress [29]. Furthermore, a 6-week Mindful Sport Performance Enhancement (MSPE) program among female student-athletes led to increased mindfulness and reduced anxiety and emotional dysregulation [30].
Mindfulness interventions have also demonstrated benefits for students with clinical conditions. College students diagnosed with major depressive disorder (MDD) experienced reductions in depressive symptoms following mindfulness-based therapy and behavioral activation [31], while a separate study found a dose-response relationship between MBCT and depression symptom reduction [32]. Spanish psychology students, U.S. psychology students with PTSD, and individuals with eating disorders in the UK reported substantial reductions in anxiety, depression, stress, and disorder-related symptoms after mindfulness training [33-35].
Moreover, mindfulness programs have shown promising results in professional and high-performance academic settings. U.S. collegiate athletes engaging in MSPE interventions demonstrated improved performance, well-being, and engagement [36]. Similarly, therapeutic radiography students reported enhanced resilience and reduced burnout following mindfulness-based interventions [37]. Healthcare students at Virginia Commonwealth University and other institutions in the U.S. benefited from MBSR and mindfulness training, reporting improvements in psychological well-being, reduced burnout, and increased empathy [38, 39]. A study on 131 undergraduate students found that Sahaj Marg Meditation (SKY) was particularly effective in reducing depression and stress, further supporting the role of mindfulness-based interventions in fostering emotional intelligence and mental health [40]. Additionally, brief, targeted in-person MBSR programs have been shown to improve awareness of medical errors [41], reduce cognitive load in high-pressure fields [42], and mitigate maladaptive behaviors, such as problematic drinking [43].
Despite these well-documented benefits, traditional in-person MBSR interventions face certain limitations (Table 3). Low adherence rates, accessibility issues, and scheduling conflicts often contribute to high dropout rates, reducing the overall effectiveness of these interventions. These challenges underscore the need for alternative or supplementary delivery methods to ensure broader participation and sustained engagement. Exploring hybrid or digital mindfulness programs may provide a more flexible and scalable approach, allowing students to integrate mindfulness practices into their academic and personal routines without the constraints of in-person attendance.
| Source | Population of Study | Intervention Duration | Outcomes |
|---|---|---|---|
| [17] | 41 college students (LMICs) | 8-week MBSR | Reduced stress, and improved brain activity |
| [18] | 99 university students and staff | 8-week MBSR (various settings) | Enhanced mental health, well-being, and nature connectedness |
| [19] | 72 nursing students (Qom University) | 8-week MBSR | Reduced stress, improved mental well-being (COVID-19 pandemic) |
| [21] | 23 Brazilian university students | 8-week MBSR | Significant stress reduction, and improved quality of life |
| [22] | 50 South Korean nursing students | 8-week MBSR | Reduced depression, anxiety, stress, and improved mindfulness |
| [23] | 288 Norwegian medical/psychology students | Modified MBSR | Reduced neuroticism, and psychological distress |
| [24] | 293 MBA students from four business schools | 20 weeks MBSR | Mindfulness scores increased, stress levels decreased, and higher mindfulness predicted better case study performance, with stress mediating this effect. |
| [25] | 96 Thai technical college students | 3-month mindfulness meditation | Reduced anger and violent behavior |
| [26] | 538 Australian nursing students | Mindfulness (duration unspecified) | Stress reduction, influenced by resilience, self-efficacy, and social support |
| [27] | 622 Italian nursing students | Mindfulness (duration unspecified) | Reduction in psychological distress and stress levels |
| [28] | 103 healthcare students | Multi-modal mindfulness (duration unspecified) | Reduced stress, anxiety, depression; enhanced well-being and resilience |
| [29] | 66 university students (U.S.) | Brief mindfulness meditation | Enhanced stress coping during social evaluative stress |
| [30] | 60 female student-athletes (U.S.) | 6-week MSPE program | Improved mindfulness, reduced anxiety, and emotional dysregulation |
| [31] | 50 college students with MDD | Mindfulness-based therapy and behavioral activation | Reduced depression symptoms |
| [32] | 60 undergraduate students with MDD | MBCT (duration unspecified) | Reduced depression symptoms, dose-response relationship identified |
| [33] | 51 Spanish psychology students | Mindfulness training (duration unspecified) | Reduced stress, anxiety, and depression |
| [34] | 39 females with eating disorders (UK) | Mindfulness meditation (duration unspecified) | Reduced eating disorder symptoms |
| [35] | 378 U.S. psychology students with PTSD | Mindfulness (duration unspecified) | Reduced PTSD avoidance symptoms |
| [36] | 65 U.S. collegiate athletes | MSPE intervention (duration unspecified) | Improved performance, well-being, and engagement |
| [37] | 14 therapeutic radiography students | Mindfulness (duration unspecified) | Reduced burnout, and enhanced resilience |
| [38] | Healthcare students (Virginia Commonwealth) | Mindfulness (duration unspecified) | Improved psychological well-being, reduced burnout |
| [39] | 16 healthcare students (U.S.) | MBSR training (duration unspecified) | Reduced anxiety, burnout, and increased empathy |
| [40] | 131 undergraduate students (U.S.) | SKY, MBSR, Emotional Intelligence (duration unspecified) | SKY showed significant improvements in depression, mental health, and stress |
| [41] | 78 Turkish nursing students | Brief MBSR (duration unspecified) | Increased awareness of medical errors |
| [42] | 72 healthcare students (Morocco) | Brief MMTP | Reduced anxiety, cognitive load, and improved teamwork |
| [43] | 293 MBA students (Slovenia) | Mindfulness (duration unspecified) | Enhanced decision-making skills, self-efficacy, and reduced stress |
| [44] | 207 U.S. college drinkers | Brief mindfulness intervention | Reduced drinking urges and negative affect |
| [45] | 80 university students (Germany) | 12-week MBST | Reduced stress, improved autonomic regulation |
3.1.2. Digital (App-Based, Online) Interventions
With the advancement of technology, digital MBSR programs have gained popularity to enhance accessibility and flexibility. These interventions are delivered through smartphone apps, online platforms, or virtual sessions, allowing university students to engage in mindfulness training at their own pace. Research suggests that digital MBSR interventions provide similar mental health benefits to traditional in-person programs. For instance, a study using the Mind Space mindfulness app reported significant reductions in stress, anxiety, and depression among university students [20]. Additionally, an mHealth mindfulness intervention demonstrated improvements in sleep quality and psychological well-being among Chinese students [46], highlighting its potential to enhance the overall well-being. Another study found that brief app-based mindfulness training improved cognitive flexibility and attentional control, although its effects on executive function performance were limited [47].
Several studies further support the efficacy of digital mindfulness programs across diverse university student populations. A study involving 100 Yemeni students in China found that digital mindfulness training effectively reduced COVID-19-related fear [48]. Similarly, an online mindfulness meditation program for university students resulted in improved brain activity and cognitive functioning [49]. Among nursing students in the U.S., participation in an 8-week online mindfulness program led to reduced stress, improved mood, and enhanced cognitive functioning [50]. Furthermore, a brief online mindfulness intervention for 104 UK university students demonstrated significant reductions in stress, anxiety, and depression, suggesting that even short-term digital interventions can yield meaningful psychological benefits [51].
Despite these promising findings, digital MBSR programs face certain challenges that may impact their overall effectiveness. Studies indicate that dropout rates tend to be higher in digital interventions compared to traditional in-person programs, largely due to the lack of direct engagement with instructors, lower retention rates, and reduced social accountability. The absence of structured, face-to-face interactions may contribute to a decline in motivation and inconsistent practice among students. Additionally, while digital mindfulness interventions provide flexibility, their effectiveness may depend on individual differences in self-discipline, engagement levels, and the ability to integrate mindfulness practice into daily life without external guidance (Table 4).
3.2. Discipline-specific Variations
MBSR and other mindfulness interventions have been applied across various disciplines, yielding different outcomes depending on the target population. While the core principles of mindfulness remain consistent, discipline-specific factors such as the nature of academic stress, cognitive demands, and professional responsibilities influence how students and professionals engage with mindfulness training.
3.2.1. Healthcare and Nursing Students
Mindfulness interventions have been widely implemented among healthcare and nursing students, who often experience high levels of stress due to the demanding nature of their training and professional responsibilities. Several studies have demonstrated the effectiveness of MBSR in reducing stress and improving well-being in this group. For instance, an 8-week MBSR intervention significantly reduced stress and improved mental well-being among 72 nursing students in Qom University during the COVID-19 pandemic [19].
| Source | Population of Study | Intervention Duration | Outcomes |
|---|---|---|---|
| [20] | 50 Thai university students with depression | Mind Space app (duration unspecified) | Reduced stress, anxiety, depression, improved mindfulness |
| [46] | 101 Chinese university students | mHealth mindfulness intervention (duration unspecified) | Improved well-being, sleep quality, reduced depression, anxiety, and stress |
| [47] | 19 university students (Australia) | App-based mindfulness training | Improved attention control, and activation of the prefrontal cortex |
| [48] | 100 Yemeni students in China | Mindfulness training (duration unspecified) | Reduced COVID-19-related fear |
| [49] | 22 university students | Mindfulness meditation (duration unspecified) | Improved brain activity and cognitive functioning |
| [50] | 26 nursing students (U.S.) | 8-week online mindfulness | Reduced stress, improved mood, and enhanced cognitive functioning |
| [51] | 104 university students (UK) | Brief online mindfulness | Reduced stress, anxiety, and depression |
Similarly, an 8-week MBSR program led to reductions in depression, anxiety, and stress while enhancing mindfulness among 50 South Korean nursing students [22]. A larger study involving 622 Italian nursing students found that mindfulness training significantly reduced psychological distress and stress levels [27]. In addition, a study with 103 healthcare students reported that multi-modal mindfulness interventions effectively reduced stress, anxiety, and depression while improving well-being and resilience [28]. These findings suggest that mindfulness training is particularly beneficial for students in healthcare-related fields, where high-pressure environments contribute to chronic stress and burnout.
3.2.2. Medical and Psychology Students
Medical and psychology students also benefit from mindfulness interventions, with studies indicating improvements in psychological well-being and reductions in burnout. A study involving Norwegian medical and psychology students found that a modified MBSR program reduced neuroticism and psychological distress [23]. Similarly, a mindfulness intervention among Spanish psychology students resulted in lower levels of stress, anxiety, and depression [33]. Among psychology students with PTSD, mindfulness training helped reduce PTSD-related avoidance symptoms [38]. These findings highlight the relevance of mindfulness for students in psychologically demanding fields, where emotional resilience and mental well-being are critical for professional competence.
3.2.3. Business and Social Sciences Students
Mindfulness interventions have also been explored in business education, where stress management and decision-making skills are essential for leadership development. A study involving 293 MBA students in Slovenia found that mindfulness training enhanced decision-making abilities, improved self-efficacy, and reduced stress [24]. Similarly, a brief mindfulness meditation intervention among 66 U.S. university students enhanced their ability to cope with social evaluative stress [29]. These results suggest that mindfulness training may be particularly useful for students in competitive, high-performance environments, where stress resilience and cognitive flexibility are key to academic and professional success.
3.2.4. Student-Athletes
Mindfulness has been applied in sports psychology to improve performance and mental well-being among student-athletes. A study of 60 female student-athletes in the U.S. found that a 6-week MSPE program improved mindfulness and reduced anxiety and emotional dysregulation [30]. Another study of 65 U.S. collegiate athletes reported that MSPE interventions enhanced performance, engagement, and overall well-being [36]. These findings suggest that mindfulness can be an effective tool for managing competition-related stress and improving focus and emotional regulation among athletes.
3.2.5. Students with Mental Health Conditions
Mindfulness interventions have shown significant benefits for students with mental health conditions, particularly depression and anxiety disorders. A study of 50 college students with MDD found that a combination of mindfulness-based therapy and behavioral activation effectively reduced depressive symptoms [31]. Similarly, among 60 undergraduate students with MDD, MBCT was found to reduce depression symptoms, with a dose-response relationship observed [32]. These findings indicate that mindfulness interventions can serve as valuable therapeutic tools for managing clinical psychological conditions in university populations.
3.2.6. Technical and Specialized Disciplines
Mindfulness training has also been integrated into technical and specialized fields, where cognitive load and decision-making under pressure are critical. For instance, a study of 96 Thai technical college students found that a 3-month mindfulness meditation program effectively reduced anger and violent behavior [25]. Additionally, among 14 therapeutic radiography students, mindfulness training led to reductions in burnout and enhanced resilience [37]. These results suggest that mindfulness may be particularly beneficial in professions where emotional regulation and high-stakes decision-making play a significant role.
Mindfulness interventions demonstrate broad applicability across diverse academic and professional disciplines. While healthcare and psychology students benefit from mindfulness in managing stress and preventing burnout, business students leverage it for decision-making and leadership skills. Similarly, student-athletes use mindfulness to enhance performance and emotional regulation, while students with mental health conditions experience symptom reduction and improved well-being. The effectiveness of mindfulness across these disciplines underscores its versatility. Yet, future research should explore how interventions can be further tailored to meet the specific needs of each student group, ensuring maximum engagement and long-term impact.
3.3. Randomized Controlled Trials (RCTs) vs. Observational Studies
RCTs are considered the gold standard for evaluating interventions, as they utilize random assignment to minimize bias and establish causal relationships. Observational studies, on the other hand, offer practical insights by assessing real-world applications, though they lack the same level of control over confounding variables.
3.3.1. Findings from RCTs
RCTs have demonstrated the efficacy of mindfulness interventions across various student populations. For example, an 8-week MBSR intervention among 72 nursing students at Qom University significantly reduced stress and improved mental well-being during the COVID-19 pandemic [19]. Similarly, a study involving 99 university students and staff across various settings found that MBSR enhanced mental health, well-being, and nature connectedness [18]. In low- and middle-income countries (LMICs), 41 college students who participated in an 8-week MBSR program experienced reduced stress and improved brain activity [17]. Additional RCTs have reinforced these findings, showing significant reductions in stress, anxiety, and depression, as well as improvements in mindfulness, cognitive function, and overall well-being across diverse student groups [21, 22, 26, 37].
RCTs have also been used to investigate the effectiveness of mindfulness interventions tailored to specific populations. For instance, among 50 South Korean nursing students, an 8-week MBSR program resulted in reduced depression, anxiety, and stress while improving mindfulness [22]. Another study found that 60 undergraduate students diagnosed with MDD who underwent MBCT showed reduced depression symptoms, with a dose-response relationship identified [32]. Furthermore, 80 German university students participating in a 12-week MBST reported reduced stress and improved autonomic regulation [45].
These findings underscore the robust evidence supporting mindfulness interventions when evaluated through RCTs. The controlled nature of these studies enhances their credibility by reducing biases and ensuring comparability across intervention and control groups. However, challenges such as small sample sizes, short intervention durations, and variations in mindfulness protocols may limit generalizability.
3.3.2. Findings from Observational Studies
Observational studies complement RCTs by exploring the effectiveness of mindfulness interventions in naturalistic settings. These studies typically examine pre-existing groups or track outcomes without random assignment, making them useful for assessing long-term trends and real-world applicability.
For example, an observational study involving 622 Italian nursing students found that mindfulness interventions, regardless of duration, were associated with a reduction in psychological distress and stress levels [27]. Similarly, among 538 Australian nursing students, mindfulness training was linked to stress reduction, influenced by factors such as resilience, self-efficacy, and social support [26]. A study involving 103 healthcare students demonstrated that multi-modal mindfulness programs contributed to reduced stress, anxiety, and depression while enhancing well-being and resilience [28].
Observational studies have also highlighted the potential benefits of digital mindfulness interventions. For instance, an mHealth mindfulness intervention among 101 Chinese university students improved sleep quality, well-being, and reduced symptoms of depression, anxiety, and stress [46]. Additionally, an app-based mindfulness training study in Australia showed improved attentional control and activation of the prefrontal cortex, which is linked to cognitive performance [47].
Despite their advantages, observational studies are inherently limited by potential biases, such as self-selection effects and confounding variables. Unlike RCTs, these studies cannot establish direct causality, making it difficult to determine whether mindfulness training alone accounts for observed improvements. Nevertheless, they provide valuable insights into how mindfulness interventions function in everyday student environments. While both RCTs and observational studies contribute to understanding mindfulness interventions, their strengths and limitations must be considered (Table 5).
| Aspect | RCTs | Observational Studies |
|---|---|---|
| Causal inference | Strong, due to randomization | Weaker, as confounders may exist |
| Control over variables | High | Low |
| Generalizability | Can be limited due to controlled settings | Higher applicability in real-world contexts |
| Sample size | Often small to medium | Can be larger, covering diverse populations |
| Flexibility | Standardized protocols | More adaptable to real-life conditions |
| Bias risk | Lower, due to experimental control | Higher, due to self-selection and confounding factors |
4. DISCUSSION
4.1. Theoretical Integration of MBSR
MBSR operates within several established psychological and educational theories, providing a structured approach to managing stress and enhancing mental well-being. This systematic review integrates Cognitive Load Theory (CLT), Self-Regulation Theory (SRT), and MBCT to provide a more cohesive conceptual framework explaining MBSR’s effectiveness in university settings.
4.1.1. CLT and MBSR
University students frequently experience cognitive overload, struggling to process extensive academic material while managing external stressors. CLT posits that excessive cognitive demands impair learning efficiency and performance. MBSR mitigates these effects by enhancing attentional control, reducing intrusive thoughts, and improving working memory capacity.
Empirical evidence supports these claims. Studies indicate that MBSR participants exhibit enhanced cognitive flexibility and attentional control, leading to improved academic outcomes [25, 47]. One study found that students who practiced MBSR demonstrated a 20% increase in task efficiency and a 30% reduction in mind-wandering episodes, highlighting its role in optimizing cognitive resources. Additionally, research on business students found that MBSR participants displayed higher decision-making accuracy and reduced impulsivity, reinforcing its alignment with CLT [26]. By reducing cognitive strain, MBSR facilitates better information retention and enhanced academic performance [20, 46].
4.1.2. SRT and MBSR
SRT emphasizes the role of emotional regulation and self-control in maintaining psychological well-being. MBSR fosters self-awareness, emotional regulation, and resilience, allowing students to proactively manage stress and develop adaptive coping mechanisms.
Studies consistently show that MBSR enhances self-regulation skills, leading to lower levels of anxiety, emotional distress, and maladaptive coping behaviors [17, 22, 26]. A meta-analysis found that university students who completed an 8-week MBSR program demonstrated a 40% improvement in emotion regulation and a 35% increase in adaptive coping strategies, such as cognitive reappraisal and acceptance [21]. Furthermore, business and STEM students who engaged in mindfulness training reported significant reductions in procrastination and avoidance behaviors, indicating stronger self-regulation [24, 25]. These findings align with SRT, which suggests that enhancing self-awareness and emotional regulation leads to improved goal setting and stress resilience.
4.1.3. MBCT and MBSR
MBSR aligns closely with MBCT, particularly in reducing negative thought patterns and enhancing self-compassion among students at risk for psychological distress. MBCT integrates mindfulness techniques to disrupt cycles of rumination and promote cognitive restructuring, making it particularly effective for students with pre-existing depression and anxiety [19, 21].
Empirical studies support this link. Research shows that MBSR significantly reduces symptoms of depression and anxiety, with some studies reporting a 50% reduction in depressive symptoms among university students following an MBSR program [17, 20]. Additionally, MBSR enhances self-compassion and acceptance, key mechanisms in MBCT that contribute to long-term emotional well-being [23]. One study found that students with high levels of self-criticism experienced a 45% increase in self-compassion scores after completing an MBSR intervention [46], reinforcing MBCT’s emphasis on changing maladaptive cognitive patterns.
4.1.4. Discussion on the Theories
Gender differences in MBSR outcomes can be understood through SRT, as female students consistently reported greater reductions in stress and anxiety compared to males [17, 22, 26]. Research suggests that women are more likely to engage in self-reflective and emotion-focused coping strategies, making them more receptive to mindfulness-based interventions. However, the lower engagement of male students in MBSR highlights the need for gender-specific adaptations to improve participation and effectiveness.
Cultural differences also play a significant role in shaping MBSR outcomes. Studies indicate that Western students exhibited higher improvements in self-compassion, whereas Asian students demonstrated stronger emotion regulation benefits [20, 46]. This aligns with MBCT, which emphasizes self-compassion as a core mechanism for reducing psychological distress. In individualistic cultures, self-compassion is often encouraged, whereas collectivist cultures emphasize emotional regulation and resilience. These findings suggest that culturally tailored MBSR interventions could enhance engagement by aligning mindfulness practices with culturally preferred emotional processing styles.
Another key finding relates to MBSR’s role in cognitive load reduction, particularly among STEM students. Research shows that STEM students demonstrate notable improvements in cognitive flexibility following MBSR training but tend to have lower engagement rates compared to humanities students [25]. This aligns with CLT, as STEM students often experience high cognitive demands due to the analytical nature of their coursework. Future interventions could explore discipline-specific mindfulness techniques to improve engagement while simultaneously reducing cognitive overload.
Integrating CLT, SRT, and MBCT into MBSR research strengthens its theoretical foundation and practical application.
This pattern aligns with broader research trends, as female university students tend to report higher levels of stress, anxiety, and depression than their male counterparts [20, 52]. Consequently, women may be more likely to engage in mindfulness-based interventions such as MBSR. However, the inclusion of both genders in most studies strengthens the generalizability of the findings. At the same time, the relatively lower representation of male students in some studies raises questions about their engagement with MBSR. Research suggests that men may be less likely to seek psychological interventions and may require different engagement strategies to encourage participation [51]. Future research should explore gender-specific responses to MBSR, assess potential barriers to male engagement, and investigate whether mindfulness interventions should be tailored to different gender-based needs.
Additionally, culturally tailored MBSR interventions should be designed to align with different emotional regulation styles, particularly in collectivist cultures where emotional control is emphasized. Another key area for exploration is discipline-specific mindfulness strategies, particularly for STEM students, who may benefit from targeted techniques that address high cognitive load and analytical demands. Finally, neuroscientific validation of MBSR’s effects using EEG and fMRI could provide deeper insights into its impact on cognitive flexibility, emotional regulation, and attentional control. By addressing these areas, future research can refine MBSR interventions, ensuring greater accessibility, engagement, and long-term psychological benefits for diverse university student populations.
4.2. Implications For Future Research and Practice
A more rigorous understanding of MBSR requires not only methodological improvements but also structured integration into student support services, academic curricula, and digital platforms to maximize accessibility and engagement. While MBSR has been shown to enhance mental health, academic performance, and emotional resilience, its effectiveness depends on implementation strategies that address student engagement, institutional constraints, and sustainability challenges.
Universities should embed MBSR with student wellness programs, offering on-campus mindfulness workshops, peer-led support groups, and crisis intervention strategies in counseling services. However, low participation rates in voluntary programs remain a challenge, particularly for students experiencing high stress levels. Future research should explore mandatory or incentivized models to encourage broader engagement while ensuring flexibility and accessibility.
Integrating mindfulness into academic curricula presents an opportunity to reach more students, though discipline-specific adaptations may be necessary. Brief mindfulness exercises in lectures, elective mindfulness courses, and faculty-led mindfulness integration could improve student well-being and cognitive performance. However, institutional barriers, including faculty workload concerns and administrative resistance, must be addressed through further research on scalable implementation strategies.
Given the increasing reliance on technology, digital MBSR interventions provide an alternative to in-person programs, offering institution-sponsored mindfulness apps, online courses, and virtual coaching. However, higher dropout rates in digital interventions suggest the need for interactive and adaptive learning approaches, such as gamification, AI-driven personalization, and social accountability features. The effectiveness of these strategies remains underexplored in university settings, highlighting a need for further empirical investigation.
For long-term sustainability, universities must integrate MBSR into institutional policies and research frameworks. Regular student well-being assessments, academic credit or extracurricular recognition for mindfulness participation, and interdisciplinary collaborations between psychology, education, and neuroscience departments could strengthen the evidence base for MBSR in higher education. However, funding and administrative constraints remain key barriers, emphasizing the need for cost-effective, scalable implementation models.
A more rigorous understanding of MBSR’s effectiveness also requires methodological improvements to enhance both causal inference and real-world applicability. Future research should integrate hybrid models that combine RCT methodologies with real-world observational studies, balancing experimental control with practical insights. Additionally, the use of standardized measurement tools, such as DASS-21 and GAD-7, would improve comparability across studies. Longitudinal research is also needed to determine whether MBSR’s benefits persist beyond six months and contribute to long-term psychological resilience. Lastly, given that most studies focus on Western and Asian student populations, cross-cultural expansion is necessary to ensure MBSR’s effectiveness in diverse educational settings, accounting for cultural variations in emotional regulation and mindfulness perception. Addressing these research gaps will optimize MBSR’s accessibility, effectiveness, and long-term impact on student well-being.
While this review highlights the benefits of MBSR for cognitive flexibility, decision-making, and engagement, it does not include direct academic performance measures such as GPA or formal academic assessments. Most studies assessed academic-related outcomes indirectly through cognitive and psychological improvements. Future research should incorporate standardized academic metrics to establish a clearer link between MBSR and measurable academic success. Longitudinal studies tracking GPA, course performance, or standardized assessments could provide stronger evidence of MBSR’s impact on academic achievement.
CONCLUSION
This systematic review underscores the substantial benefits of MBSR in enhancing university students' mental health and academic performance. Findings confirm that MBSR is effective in reducing stress, anxiety, and depression while improving cognitive flexibility, emotional regulation, and self-awareness. These effects are particularly pronounced among students in high-stress academic disciplines such as healthcare, psychology, and business.
Among intervention types, traditional in-person MBSR programs have demonstrated strong, consistent results, particularly in structured university settings where guided mindfulness training fosters long-term engagement and mental health improvements. However, digital mindfulness programs, while offering greater accessibility and flexibility, face lower adherence and engagement rates, suggesting that further refinement is needed to sustain participation. Future research should explore hybrid models that integrate in-person and digital components to optimize accessibility and effectiveness.
A comparative analysis of RCTs and observational studies provides valuable insights. RCTs confirm the causal relationship between MBSR and improved mental health outcomes, reinforcing its validity as an evidence-based intervention. Observational studies highlight MBSR’s real-world applicability, demonstrating its effectiveness in diverse educational contexts. However, higher dropout rates in digital interventions and variations in study design emphasize the need for more standardized methodologies.
Theoretical frameworks further validate MBSR’s impact. CLT explains how mindfulness reduces cognitive overload, improving focus and information retention. SRT supports MBSR’s role in enhancing self-control and resilience, allowing students to manage stress more effectively. MBCT provides a framework for understanding how MBSR disrupts maladaptive thought patterns, making it particularly beneficial for students experiencing chronic stress or depression.
Despite these encouraging findings, several limitations must be addressed. The small sample sizes of many studies, along with variability in intervention duration and assessment measures, limit the generalizability of results. Additionally, most studies rely on self-reported measures, which may introduce bias. Future research should incorporate objective psychological and physiological assessments, such as neuroimaging or biomarker analysis, to validate MBSR’s effects.
Another challenge is the discipline-specific variation in engagement and effectiveness. While healthcare and psychology students show high participation rates and significant mental health improvements, STEM students demonstrate lower engagement despite cognitive benefits. Business students, on the other hand, gain improvements in decision-making and emotional regulation, highlighting the need for tailored mindfulness strategies based on academic discipline. Future research should develop discipline-specific adaptations of MBSR, ensuring its effectiveness across diverse student populations.
To enhance the long-term sustainability of MBSR’s effects, universities should integrate mindfulness training into student wellness programs and academic curricula. Institutional support, faculty-led mindfulness initiatives, and student-led mindfulness communities could help maintain engagement and normalize mindfulness practice as part of higher education culture.
In conclusion, MBSR is a highly effective intervention for improving mental well-being and academic performance among university students. However, greater emphasis on hybrid models, standardized research methodologies, and tailored discipline-specific adaptations is necessary. The integration of digital tools, institutional support, and theoretical advancements will further strengthen MBSR’s role in higher education, ensuring long-term accessibility, engagement, and psychological benefits for students worldwide.
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the paper as follows: P.X.: Contributed to the study design, data collection, analysis, and manuscript writing; S.M.S.A.: Contributed to the study design, data interpretation, and manuscript revision. Both authors have reviewed and approved the final version of the manuscript for submission.
LIST OF ABBREVIATIONS
| GAD-7 | = 7-item Generalized Anxiety Disorder scale |
| PSD | = Alpha Power Spectral Density |
| BMI | = Body Mass Index |
| SKY | = BREF Sahaj Marg Meditation |
| CD-RISC | = Connor-Davidson Resilience Short Form Scale |
| ACT | = Dispositional Mindfulness, Acceptance and Commitment Therapy |
| DLPFC | = Dorsolateral Prefrontal Cortex |
| EEG | = Electroencephalogram |
| EI | = Emotional Intelligence |
| FD | = Emotional Intelligence Fractal Dimension |
| FFMQ-SF | = Five Facet Mindfulness Short Form Questionnaire |
| fMRI | = Functional Magnetic Resonance Imaging |
| fNIRS | = Functional Near-Infrared Spectroscopy |
| LMICs | = Low-Middle-Income Countries |
| MBI-SS | = Maslach Burnout Inventory Student Survey |
| MSPE | = Mind Sports Performance Enhancement |
| MMTP | = Mindfulness Meditation Training Program |
| MBCT | = Mindfulness-Based Cognitive Therapy |
| MBIs | = Mindfulness-Based Interventions |
| MBSR | = Mindfulness-Based Stress Reduction |
| MBST | = Mindfulness-Based Student Training |
| MBTs | = Mindfulness-Based Therapies |
| PHQ-9 | = Patient Health Questionnaire |
| PSS | = Perceived Stress Scale |
| PSQI | = Pittsburgh Sleep Quality Index |
| PTSD | = Post-Traumatic Stress Disorder |
| PRISMA | = Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| ProQOL | = Professional Quality of Life Scale |
| SCS | = Self-Compassion Scale |
| SMS | = State Mindfulness Scale |
| WHOQOL-BREF | = World Health Organization Quality of Life - BREF |
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
ACKNOWLEDGEMENTS
Declared none.

