All published articles of this journal are available on ScienceDirect.

P300 Marker of Emotional Attention Bias in Health-risk Smoking Behaviors: The Specific and Distinct Roles of ASPD and Moral Identity
Authors Info & Affiliations
Abstract
Introduction
The relationship between antisocial personality disorder (ASPD), moral identity, and health-risk behaviors such as smoking in young adults reflects a complex psychosocial and neurobiological construct. This study aimed to (1) examine the predictive roles of ASPD traits and moral identity in emotional attention bias toward health-risk smoking behaviors (Model 1) and non-health risk behaviors (Model 2), and (2) investigate whether moral identity moderates the association between ASPD traits and emotional attention bias for these behaviors (Partial Correlation Models 1 and 2).
Methods
Twenty-one participants (mean age = 22 years) meeting eligibility criteria were recruited. Brain activity associated with attentional bias was measured using event-related potentials (ERPs). Participants viewed visual stimuli representing smoking-related behaviors, non-health risk behaviors, and neutral content, while P300 brain potentials were extracted following standard procedures at central-parietal regions.
Results
Moral symbolization explained 24% of the variance in attentional bias toward smoking-related stimuli in Model 1 and 26% of the variance in attention to non-health risk behaviors in Model 2, as reflected by P300 amplitude. Moral internalization significantly moderated the relationship between impulsivity and attention bias toward smoking stimuli, as indicated by P300 latency (p = 0.03). Callous-unemotional traits were also significantly associated with attentional bias for smoking-related behaviors, influenced by moral internalization (p = 0.03).
Discussion
Findings indicate that moral symbolization robustly predicts attentional responses to both risky and non-risky cues, while moral internalization buffers impulsivity and callous-unemotional traits in shaping smoking-related biases. These results highlight the neurocognitive role of moral identity in regulating risky attentional patterns, extending prior research on moral–emotional regulation.
Conclusion
Strengthening moral identity could serve as an intervention strategy to reduce attentional biases toward health-risk behaviors, supporting the development of targeted programs for healthier decision-making. Replication with larger, more diverse samples is warranted.
1. INTRODUCTION
The relationship between antisocial personality disorder (ASPD), moral identity, and health risk behavior such as smoking in young people highlights a dynamic interplay of psychological, social, and neurobiological factors. ASPD, characterized by impulsivity, disregard for social norms, and lack of empathy, often predisposes young individuals to health-compromising behaviors such as substance abuse, risky sexual activities, and reckless decision-making [1]. These behaviors stem from deficits in self-regulation and impaired emotional processing linked to dysfunctions in brain regions like the amygdala [2, 3]. On the other hand, moral identity refers to the degree to which being a moral person is central to one’s self-concept [4], which in turn helps in shaping positive and healthy behaviors. Unsurprisingly, young individuals with ASPD may exhibit a weak moral identity [5], resulting in limited motivation to engage in health-conscious or socially responsible actions. The empathy deficit commonly observed in ASPD [6], disrupts the internalization of moral values that typically guide prosocial and health-promoting behaviors [7]. Consequently, the interaction of ASPD traits and a diminished moral identity significantly amplifies the risk of negative health behaviors [8], creating a pattern of maladaptive choices. Interventions targeting moral development, emotion regulation, and social influence are essential for mitigating these health risks and fostering better outcomes for affected youth.
Moral identity may influence the relationship between ASPD and health-compromising behaviors, such as smoking, which is strongly linked to ASPD due to tendencies toward risk-taking and immediate gratification [1]. However, the strength of this association can vary depending on the individual’s moral identity. A strong moral identity can serve as a protective factor against smoking by enhancing self-regulation and discouraging behaviors perceived as harmful or irresponsible [9]. Conversely, a weak moral identity may strengthen the connection between ASPD and smoking, as it offers less internal motivation to counteract the impulsive and risk-taking tendencies linked to ASPD. Interventions that emphasize moral values and accountability could help mitigate the impact of ASPD traits on smoking, promoting healthier decision-making.
Smoking behavior among young people is a complex issue influenced by social, psychological, and moral factors. Social pressures, such as peer influence and the glamorization of smoking in media, often drive youth to smoke as a means of gaining social acceptance, expressing independence, or challenging authority [10]. Socio-economic factors further contribute, with disadvantaged communities experiencing higher rates of smoking due to stress, lack of education, and targeted marketing by the tobacco industry [11]. From a moral perspective, smoking raises questions about personal responsibility, addiction, and the ethical implications of supporting industries tied to significant health consequences. Young people with a strong moral identity, encompassing both internalized values and outward moral actions, are more likely to avoid smoking, perceiving it as harmful to themselves and others [12]. Additionally, societal stigma around smoking can deter the behavior but may also alienate those who smoke, potentially reinforcing rebellious tendencies [13]. Effective prevention should integrate health education, moral development, and policies that address both individual behaviors, and while considering broader social influences.
The field of neuroscience sheds light on the role of ASPD and moral identity in predicting health-compromising behaviors by examining the brain mechanisms underlying emotional regulation, moral reasoning, and impulse control [14]. In individuals with ASPD, abnormalities in the prefrontal cortex (linked to decision-making and self-regulation), the amygdala (responsible for emotional processing and fear of consequences), and the default mode network (associated with moral reasoning) result in diminished impulse control, empathy, and awareness of long-term consequences, making them more prone to risky behaviors [15]. A strong moral identity can act as a buffer, promoting prosocial behavior and suppressing harmful impulses. However, when moral identity is weak and coexists with ASPD, the neural systems supporting self-regulation and moral reasoning may be compromised, increasing the likelihood of health-risk behaviors such as substance abuse [16]. This interplay highlights how deficits in specific brain networks can predict vulnerability to health-compromising actions.
This study aims to answer two main questions. First, what are the predictive factors-specifically antisocial personality disorder (ASPD) traits and moral identity-for emotional attentional bias in two models: the health-risk smoking model and the non-health-risk model, and do these predictive factors differ between the two models? Second, what is the strength of the relationship between ASPD domains and emotional attentional bias when exposed to health-risk smoking stimuli and non-health-risk stimuli, after controlling for moral identity?
2. METHODS
2.1. Research Design
This was a quantitative, analytical cross-sectional study, conducted in the Neuroscience Laboratory and employed the event-related potential (ERP) technique to investigate neurocognitive processes. ERPs are brief changes in the electroencephalogram (EEG) recorded on the scalp that occur in response to specific events, such as sensory stimuli, cognitive tasks, or motor actions. This method allows for the precise temporal measurement of brain activity, providing insights into the timing and neural mechanisms underlying cognitive and emotional processes [17]. EEG was utilized as a non-invasive tool to capture electrical activity in the brain. It offers a valuable approach for understanding neurobiological imbalances and investigating neurotransmission, particularly in conditions associated with altered cognitive or emotional functioning, such as emotional attention bias.
2.2. Participants
The young adult age group (average age 22 ± 2.1 years) was the primary focus of this study. To determine the appropriate sample size for the multiple linear regression analysis with two predictors (ASPD traits and moral identity), we initially estimated the required number of participants using GPower. Based on a previously reported R2 value of 0.24, Cohen’s f2 effect size was calculated as 0.32, indicating a medium-to-large effect size. With an alpha level of 0.05, desired power of 0.80, and two predictors, the minimum required sample size was estimated to be 28 participants. However, due to practical constraints, the current study included 21 participants. A post hoc power analysis using G-Power indicated that, with the given sample size, alpha level, and effect size, the achieved statistical power was approximately 0.71. While this is slightly below the conventional threshold of 0.80, it still reflects an acceptable level of power for detecting medium-to-large effects. Most participants were Malays and predominantly Muslims (ages ranged from 20 to 24 years old), with only a small number of non-Malays included. Approximately 70% (n=14) of the participants were female, resided in the Kota Bharu district of Kelantan, a suburban city in West Malaysia. The majority had a similar educational background, with most having completed high school. Some of them were employed. Participants with visual impairments used glasses to ensure clear vision while responding to visual stimuli. All participants were right-handed and reported no history of neuropsychiatric or chronic medical conditions.
2.3. Research Procedure
Information about the study was shared via social media to reach potential participants, utilizing a convenient sampling method for recruitment. Individuals who met the inclusion criteria-specifically, being right-handed, having no history of neuropsychiatric disorders or chronic medical conditions, and possessing normal or corrected-to-normal vision-were invited to participate in the study conducted at the Neuroscience Laboratory, Specialist Hospital, Universiti Sains Malaysia. Participants with a history of head injury resulting in loss of consciousness or seizures (including drug-induced seizures) were excluded from the study. They were given detailed information about the study procedures, and informed consent was obtained from each participant. The study protocol received approval from the Human Ethics Committee (approval number: USM/JEPeM/ 19070388) in compliance with the Helsinki Declaration 2013. Before beginning the EEG recordings in the laboratory, the level of the participants’ trait of moral identity (using the Moral Identity Scale) and their antisocial personality scores (using the Antisocial Personality Disorder Scale) were assessed. Additionally, sociodemographic information was also collected.
2.3.1. Moral Identity
This study used the Malay Version of Moral Identity Scale (MIS) to measure the degree of internalization and symbolization traits of the participants. Internalization refers to an intrinsic value deeply integrated into the participant’s self-concept, while symbolization reflects an external value expressed through actions that project a social identity based on moral traits [18]. Participants’ intrinsic values were assessed using three items, such as “It would make me feel good to be a person who has these characteristics”. The external values were measured through five items, including statements similar to “I often wear clothes that identify me as having these characteristics”. Participants rated the items using a 7-point Likert scale, ranging from 1 (completely disagree) to 7 (completely agree). The Malay version of the MIS has been psychometrically validated and demonstrates acceptable reliability and construct validity in assessing moral internalization and symbolization among Malaysian youth [19].
2.3.2. Antisocial Personality Disorder
The self-report Malay version of the APSD was used to assess the psychopathic traits among the study participants. The APSD is a 20-item self-report behavior rating scale designed to assess antisocial traits in individuals, particularly in youth populations [20]. The items are scored on a 3-point Likert scale ranging from 0 (Not at all true), 1 (Sometimes true), to 2 (Definitely true). Factor analysis has identified three dimensions within the APSD: narcissism, impulsivity, and callous-unemotional traits. This instrument has shown effectiveness in identifying individuals with more severe, chronic, and violent behavioral patterns [21], as well as those exhibiting deficiencies in emotional functioning [22]. Previous studies have reported adequate internal consistency for the total APSD score, with Cronbach's alpha ranging from 0.78 to 0.81, while subscale alphas ranged from 0.50 to 0.68 [23]. In this study, the total score for APSD ranges from 0 to 40, with a higher score indicating higher levels of psychopathic traits. The internal consistency of the scale was found to be 0.69 for the total score, with subscale alphas ranging between 0.41 to 0.68
2.4. EEG Recording
A controlled laboratory environment was ensured to minimize external noise and artifacts that could interfere with EEG recordings. Participants were seated comfortably in a sound-attenuated, dimly lit room to maintain focus and reduce distractions during data collection. Visual stimuli were presented on a computer screen, and participants’ responses were recorded using a response box to ensure precise synchronization with EEG data. This setup aimed to achieve high temporal resolution in capturing brain activity, providing a robust framework for examining the relationship between attentional bias, emotional stimuli, and associated neurocognitive processes.
During the ERP session, participants were shown a series of images categorized into health-risk smoking behaviors, non-health-risk behaviors, and neutral images (geometric shapes) displayed on a computer screen. EEG brainwaves were recorded using a NetAmps 300 amplifier with high input impedance. A 128-channel HydroCel Geodesic Sensor Net was fitted on the participants’ heads to monitor their emotional and cognitive responses in real time.
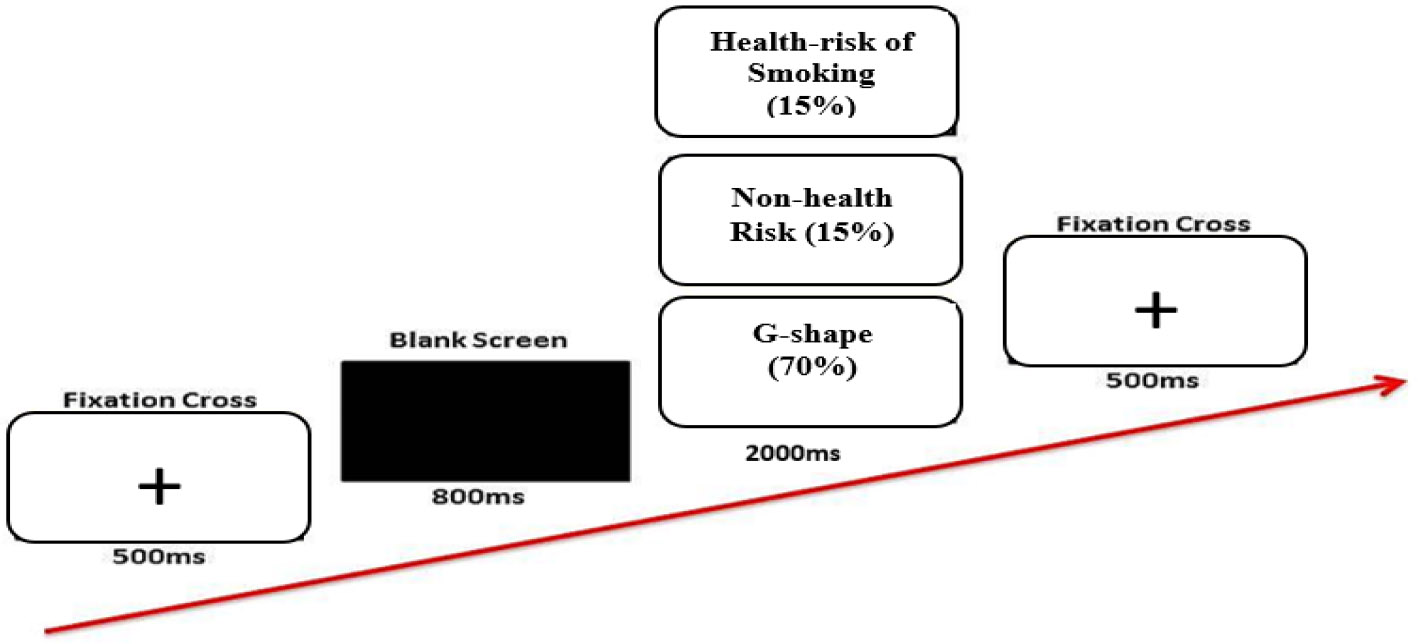
The experimental procedure is illustrated in Fig. (1) [24]. Each trial began with a fixation cross (+) displayed at the center of the monitor for approximately 500 ms, followed by a blank screen shown for 800 ms. Subsequently, a visual image was presented for 2000 ms. The images were displayed following the oddball paradigm, in which sequences of repetitive stimuli were occasionally disrupted by a deviant stimulus. In this experiment, non-target images (geometric shapes) appeared more frequently than target images, with a ratio of 70% non-targets to 30% targets, equivalent to a 1:1:3 distribution. A total of 200 image trials were presented in random order, with each category repeated three times. Each trial began with the fixation cross and proceeded as described until all 200 trials were completed. This structured approach ensured consistency and reliability in the data collection process.
2.5. Visual Stimuli
The experiment utilized two categories of images: those depicting health-risk smoking behavior and non-health-risk behaviors (target images comprising 30% of the total) and neutral images (non-target images comprising 70%). An example of images is exhibited in Fig. (2) [24]. The operational definition used to describe the images is as below (Table 1):
Event-related potential procedure. Reproduced from Shaharum MH, Yusoff N, Reza F, Ismail R, Kueh YC, Azman A. Moral internalization influences the attentional bias to smoking and non-smoking stimuli in Malaysian youth. Med. & Health. 2024;19(1):173–191. Licensed under CC BY-NC 4.0.
| A | Health risk (deviant) smoking behaviour stimuli | Images of young people smoking cigarettes or using tobacco-based products. |
| B | Non-health risk (normative) behaviour stimuli | Images of young people engaging in healthy activities, such as jogging, cycling, swimming, and other sports, instead of smoking. |
| C | Neutral stimuli | Geometry – serves as repetitive stimuli that are occasionally disrupted by deviant or normative stimuli (as depicted in A and B). |
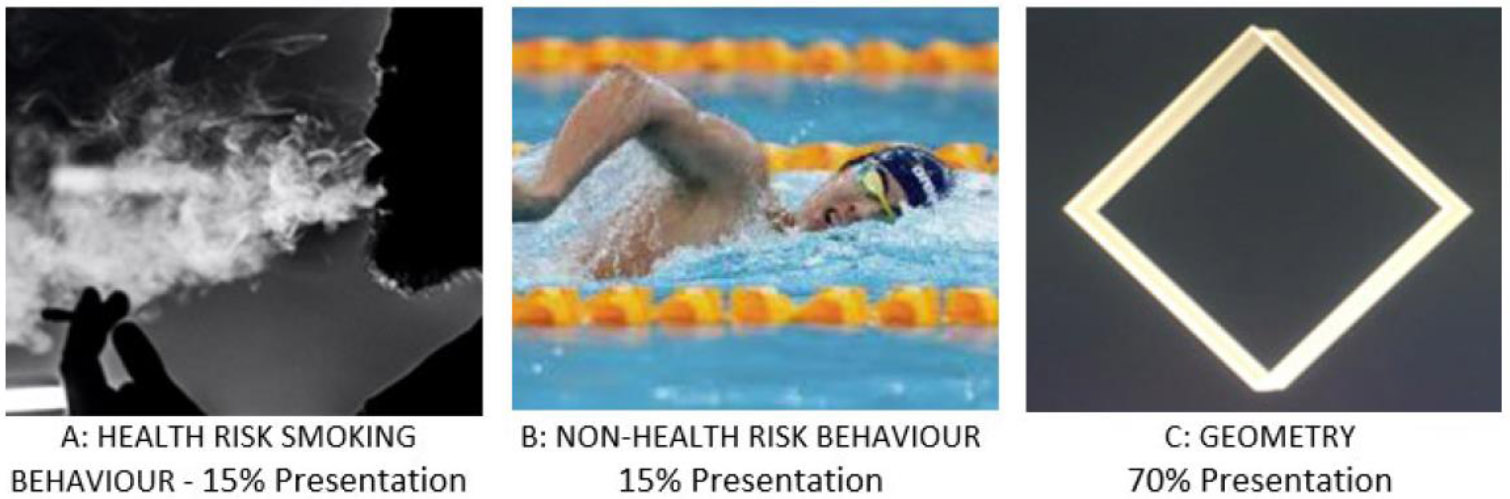
Different categories of visual presentation in the odd-ball paradigm. Adapted from Shaharum MH, Yusoff N, Reza F, Ismail R, Kueh YC, Azman A. Moral internalization influences the attentional bias to smoking and non-smoking stimuli in Malaysian youth. Med. & Health. 2024;19(1):173–191. Licensed under CC BY-NC 4.0.
The objective was to explore the neural mechanisms underlying attentional bias toward health-risk smoking and non-health-risk behaviors, as influenced by the domains of moral identity and antisocial personality disorder. All images were sourced from the internet and are copyright-free.
The content validity of the images was assessed by two psychologists and one public health practitioner, who rated a series of health-risk (deviant) smoking behavior and non-health-risk (normative) images using the following scale: 1 = not relevant, 2 = somewhat relevant, 3 = quite relevant (denoted as X), and 4 = highly relevant (also denoted as X) [25]. The Individual Content Validity Index (I-CVI) was used to evaluate the validity of each image based on the ratings of 3 or 4, attributed by the evaluators. The I-CVI value was calculated using the formula: Number of X ratings (scores of 3 or 4) / Total Number of Evaluators.
For the final analysis, 20 images (10 depicting smoking and 10 non-health risk behaviors) with an I-CVI score of 1 were selected. An I-CVI score of 1 represents an acceptable threshold for content validity. To reduce technical bias, the brightness and dimensions of all images were standardized.
2.6. Raw Data Extraction and Analysis
ERP data was recorded using Ag/AgCl electrodes with carbon pellets encased in sponges, connected via a 1-meter insulated lead wire to a Hypertronics-compatible, gold-plated pin. Following the international 10/20 system, scalp sites across five brain regions were selected for analysis: fronto-parietal (Fp1, Fp2), frontal (F3, F4, F7, F8, Fz), central (C3, C4, Cz), temporal (T3, T4, T5, T6), parietal (P3, P4, Pz) and occipital (O1, O2). The Fz, Cz, and Pz electrodes, corresponding to the P300 component, were specifically selected for analysis. These midline electrodes are significant in event-related potential (ERP) studies as they correspond to key brain regions involved in cognitive and neural processes. Fz, Cz, and Pz reflect neural activity in the prefrontal, central, and parietal regions of the brain, respectively, which are crucial for attention, decision-making, working memory, and the integration of sensory information. The P300 component is indicative of the brain’s ability to allocate attentional resources to stimuli, with a larger P300 reflecting a greater focus of attention on a task-relevant stimulus. Additionally, the P300 is associated with the evaluation of stimulus significance, indicating how the brain categorizes and responds to relevant versus irrelevant stimuli, and reflecting cognitive processes involved in decision-making. Compared to other ERP components, the P300 (or P3) is one of the most well-understood and reliable, consistently appearing in response to rare, task-relevant, or emotionally salient stimuli-particularly within oddball paradigms.
Before statistical analysis, the raw ERP data were processed using standardized steps to extract specific components. A 0.3-30 Hz bandpass filter was applied to the raw EEG signals to remove noise from electrical interference and muscle activity. The data were then segmented, aligning the epochs to 200 milliseconds before stimulus onset and extending to 1000 milliseconds post-stimulus, with a 45-millisecond offset. Artifact detection was performed to identify and remove ocular artifacts, such as blinks and eye movements. Channels with excessive noise (approximately 20% of recordings across segments) were interpolated using data from surrounding intact electrodes. The waveforms were then averaged to enhance the signal-to-noise ratio. The data were converted into the 10-20 EEG montage and baseline-corrected. Finally, the processed waveforms were combined, averaged, and converted into numerical data for statistical analysis.
To address the first objective, a linear regression analysis (using both the enter and stepwise methods) was conducted. In Model 1, the independent variables, i.e. moral identity (internalization and symbolization) and ASPD domains (narcissism, impulsivity, and callous-unemotional traits), were hypothesized to predict emotional attention to health-risk (deviant) smoking behavior stimuli. In Model 2, the same independent variables were hypothesized to predict emotional attention to non-health-risk (normative) behavior stimuli.
To address the second objective, a partial correlation analysis was conducted. Emotional attention bias for both health-risk smoking behavior and non-health risk behavior stimuli was indexed by the P300 ERP component measured at the Fz, Cz, and Pz electrodes. All analyses were performed using the IBM Statistical Package for the Social Sciences (SPSS).
3. RESULTS
The Pz electrode indicates a significant brain’s processing of stimulus information. The amplitude and latency of the P300 component, particularly at the Pz electrode, demonstrated distinct roles in the relationship between independent variables (ASPD domains, moral identity) and dependent variables (emotional attention processing of health risk smoking behaviors and non-health risk behavior stimuli). The two key findings emerged from the analysis as below:
3.1. Linear Regression Model
Only symbolization significantly predicted emotional attention in both models; the health-risk smoking behavior model (β = 0.49, t = 2.5, p = 0.02) and the non-health behavior model (β = 0.51, t = 2.6, p = 0.02), as indicated by the P300-Pz amplitude. Specifically, symbolization accounted for 24% of the variance in emotional attention to smoking-related stimuli in the health-risk smoking behavior model. Similarly, symbolization explained 26% of the variance in emotional attention to non-health risk behavior stimuli in the non-health risk behavior model. Other predictors (i.e., narcissism, impulsivity, callous-unemotional, moral internalization) did not significantly predict emotional attention in either model i.e., the health-risk smoking behavior and the non-health behavior model. These results were derived using the stepwise method, while the enter method did not yield any significant findings across all analyses (see Table 2 for a detailed breakdown).
| Predictors | Narcissism (N=21) |
Impulsivity (N=21) |
Callous-Unemotional (N=21) | Moral Internalization (N=21) |
Moral Symbolization (N=21) |
|---|---|---|---|---|---|
| MEAN (SD) | 2.0 (1.4) | 3.3 (1.9) | 10.0 (1.5) | 20.2 (3.8) | 16.4 (1.9) |
| Central Parietal (Pz) | |||||
| Standardized Coefficients Beta (Enter) | 0.05- AS 0.26 – ANS 0.15 - LS -0.15 - LNS |
0.23- AS -0.15 – ANS -0.34 – LS -0.17 - LNS |
-0.17- AS 0.37 – ANS -0.27 – LS -0.29 - LNS |
0.06- AS -0.28 – ANS 0.48 – LS 0.122 - LNS |
0.46- AS 0.45 – ANS -0.04 – LS 0.15 - LNS |
| R2 (Enter) | 0.29 (NS) – AS; 0.48 (NS) – ANS; 0.47 (NS) – LS; 0.20 (NS) - LNS | ||||
| Standardized Coefficients Betaa/Beta Inb (Stepwise) | 0.09b (Excl) – AS 0.24b (Excl) – ANS LS1 LNS1 |
0.16b (Excl) – AS 0.03b (Excl) – ANS LS1 LNS1 |
-0.05b (Excl) – AS 0.25b (Excl) – ANS LS1 LNS1 |
0.06b (Excl) – AS -0.32b (Excl) – ANS LS1 LNS1 |
0.49a (Predictor) – AS 0.51a (Predictor) – ANS LS1 LNS1 |
| R2 (Stepwise) | - | - | - | - | 0.24 (p=0.02) - AS 0.26 (p=0.02) - ANS |
| Central Brain (Cz) | |||||
| Standardized Coefficients Beta (Enter) | -0.17- AS 0.20 – ANS 0.21 – LS 0.02 - LNS |
-0.34- AS -0.22 – ANS -0.21 – LS -0.38 – LNS |
0.28- AS 0.07 – ANS 0.19 - LS 0.16 - LNS |
0.16- AS 0.52 – ANS 0.39 – LS 0.24 - LNS |
0.20- AS 0.16 – ANS 0.07 – LS 0.54 - LNS |
| R2 (Enter) | 0.17 (NS) - AS; 0.24 (NS) – ANS; 0.19 (NS) – LS; 0.29 (NS) - LNS | ||||
| Standardized Coefficients Betaa/Beta Inb (Stepwise) | AS1 ANS1 LS1 LNS1 |
AS1 ANS1 LS1 LNS1 |
AS1 ANS1 LS1 LNS1 |
AS1 ANS1 LS1 LNS1 |
AS1 ANS1 LS1 LNS1 |
| R2 (Stepwise) | None | None | None | None | None |
| Central Frontal (Fz) | |||||
| Standardized Coefficients Beta (Enter) | -0.11- AS 0.10 – ANS -0.09 – LS -0.01 - LNS |
-0.32- AS 0.01 – ANS 0.05 – LS -0.01 LNS |
0.39- AS 0.03 – ANS -0.18 – LS -0.06 - LNS |
0.19- AS -0.13 – ANS 0.34 – LS 0.24 - LNS |
0.62- AS -0.07 – ANS -0.22 – LS -0.13 - LNS |
| R2 (Enter) | 0.37 (NS) – AS; 0.03 (NS) – ANS; 0.21 (NS) – LS; 0.10 (NS) - LNS | ||||
| Standardized Coefficients Betaa/Beta Inb (Stepwise) | AS1 ANS1 LS1 LNS1 |
AS1 ANS1 LS1 LNS1 |
AS1 ANS1 LS1 LNS1 |
AS1 ANS1 LS1 LNS1 |
AS1 ANS1 LS1 LNS1 |
| R2 (Stepwise) | None | None | None | None | None |
LS: Latency for smoking pictures stimuli
ANS: Amplitude for non-smoking pictures stimuli
LNS: Latency for non-smoking pictures stimuli
ANS1: Variable was excluded in regression equation for stepwise method
LS1: Variable was excluded in regression equation for stepwise method
NS: Not Significant
Excl: Excluded.
3.2. Partial Correlation Model
In this partial correlation analysis, the significant findings and their corresponding zero-order correlations were reported. Of the 18 partial correlation models analyzed, only two demonstrated significant results.
Based on the Pearson correlation coefficient r, the zero-order correlation analysis revealed a moderate positive linear relationship for the association between impulsivity and attentional bias toward health-risk smoking behavior stimuli (r = 0.41, ns), as indexed by P300 latency at the Pz electrode. Similarly, callous-unemotional traits showed a moderate positive linear relationship with attentional bias to health-risk smoking behavior stimuli (r = 0.39, ns), which was also indexed by P300 latency at Pz. However, the correlations between impulsivity and callous-unemotional traits with moral internalization were very weak (r = 0.09, ns and r = 0.11, ns, respectively). Moral internalization, on the other hand, showed a moderate positive linear relationship with attentional bias to health-risk smoking behavior stimuli, indexed by P300 latency at Pz (r = 0.42, ns).
In the subsequent analyses, partial correlation analysis was conducted to examine the relationship between impulsivity and callous-unemotional traits (independent variables) and attentional bias to health-risk smoking behavior stimuli (dependent variable, indexed by P300 latency at Pz), while controlling for moral internalization. The results indicated a significant negative partial correlation between impulsivity and attentional bias to health-risk smoking behavior stimuli, controlling for moral internalization, as reflected in P300 latency at the Pz electrode (r = -0.50, p = 0.03). Similarly, callous-unemotional traits also showed a significant negative partial correlation with attentional bias to health-risk smoking behavior stimuli, when moral internalization was controlled (r = -0.48, p = 0.03). However, no significant partial correlations were found between impulsivity or callous-unemotional traits and attentional bias to non-health-risk behavior stimuli when controlling for moral internalization, as indexed by P300 latency at the Pz electrode. A detailed breakdown of these results is presented in Fig. (3).
4. DISCUSSION
The P300 ERP component is a critical marker in social, moral, and psychological research, serving as an indicator of cognitive processes such as attention, decision-making, and evaluation [26]. In the context of social and moral psychology, the P300 is particularly valuable for understanding how individuals process stimuli that evoke moral judgments, social norms, or emotional responses. This component is characterized by a large, positive wave occurring approximately 300 milliseconds after the presentation of relevant or unexpected stimuli, reflecting the brain’s allocation of attention and the evaluation of stimulus relevance [27]. In moral and social contexts, the P300 has been associated with the brain’s response to stimuli that challenge personal values, social norms, or ethical considerations, making it a vital tool for studying moral violations, fairness, and behavioral assessments.
The central parietal region (Pz) demonstrated significant activation during the processing of health-related information, as indicated by the P300 ERP component. The parietal cortex plays a crucial role in attention, sensory integration, and cognitive evaluation, which are key processes in responding to health-related stimuli. The P300 reflects the allocation of cognitive resources to relevant or unexpected stimuli, with heightened responses typically observed in regions that integrate sensory information, such as the parietal lobe [28]. Health-related information often requires evaluative decision-making, resulting in stronger activation of these regions as individuals assess the personal relevance and implications of such stimuli. In contrast, the central (Cz) and frontal (Fz) brain regions are more involved in early-stage processing (e.g., N200) and higher-order functions such as conflict monitoring, action planning, or cognitive control, which contribute less directly to the evaluation and integration of health-related information. This explains the pronounced involvement of the Pz region in processing such stimuli, as it integrates cognitive appraisals and attention, leading to increased P300 amplitude.
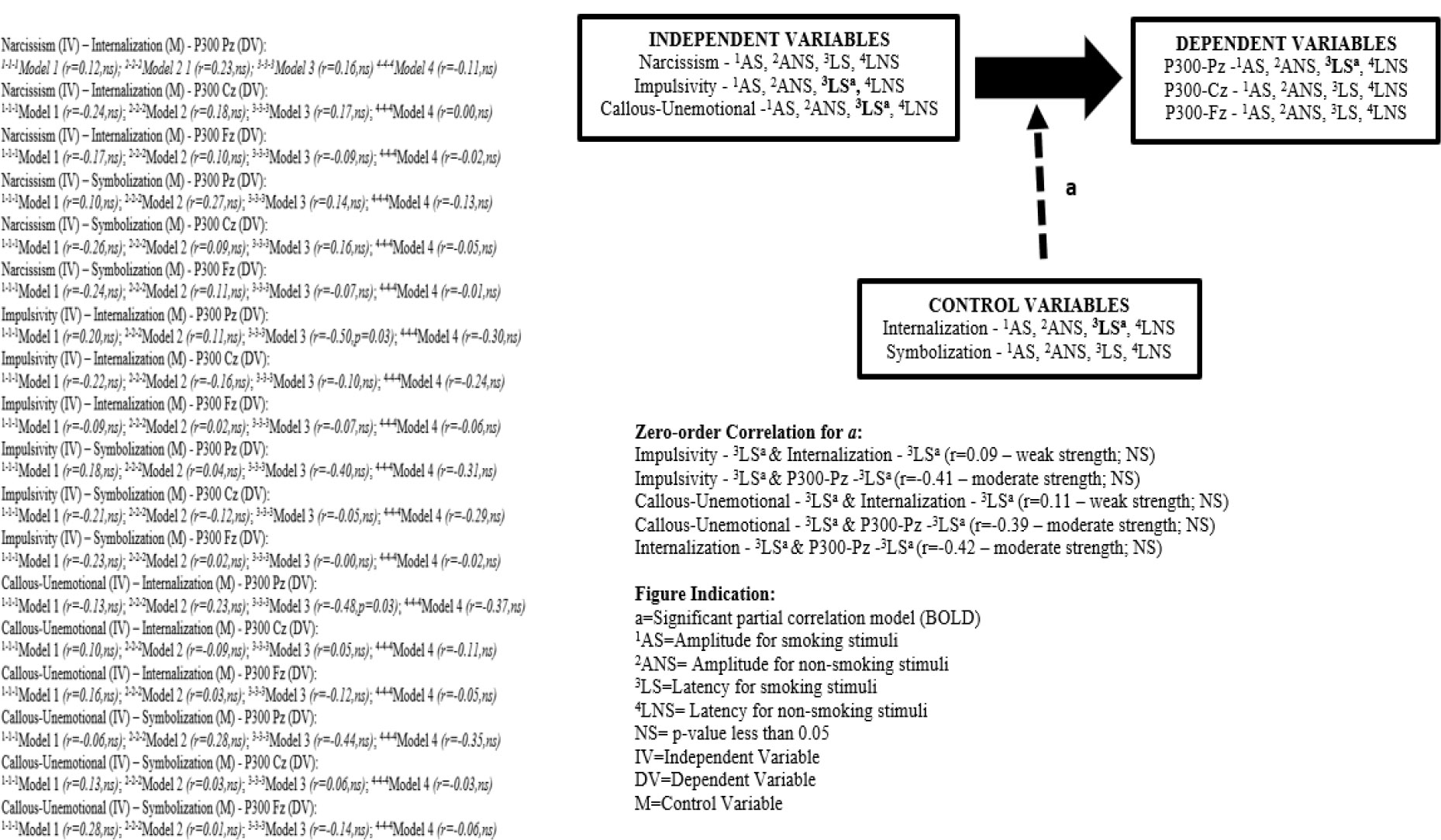
The partial correlation model of moral identity as a control variable (M) for the connection between ASPD (IV) and the attentional bias to smoking behaviour (V).
The contrasting roles of moral symbolization and moral internalization in predicting emotional attention to health-risk smoking behavior and non-health risk behavior stimuli stem from the distinct psychological constructs they represent and their differential influences on cognition and behavior. Moral symbolization reflects the external expression of moral values and a concern with how one’s behavior aligns with societal norms [7]. This makes individuals more sensitive to visual stimuli, such as health-risk smoking behavior or non-health risk behavior images, which carry strong social and cultural connotations. Such stimuli align with visible moral judgments, including the stigmatization of smoking or the virtue associated with non-smoking behaviors, resulting in heightened attention.
In contrast, moral internalization pertains to deeply held, intrinsic moral values that guide behavior irrespective of external validation [9]. Individuals with high moral internalization may not exhibit heightened emotional responses to these specific cues, as their responses are guided more by abstract principles and internalized beliefs than by external, situational stimuli. The context-dependent nature of moral symbolization likely drives its predictive power in engaging attention to these images, particularly in cultures where smoking behaviors are morally charged and tied to societal perceptions. The study design and the nature of the stimuli, which evoke external social judgments more effectively than deep ethical reflections, further explain why moral symbolization had a stronger influence, while moral internalization did not significantly predict responses to these visual stimuli.
The absence of a confounding effect for moral symbolization may stem from its focus on outward expression of moral values and conformity to societal norms, which are less relevant to the intrinsic cognitive and emotional regulatory processes underlying impulsivity and callous-unemotional traits. In contrast, moral internalization, reflecting deeply held moral principles, aligns more closely with these processes, enabling it to influence the relationship between these traits and attentional bias to health-risk smoking behavior stimuli. Smoking stimuli likely carry a greater moral and emotional weight, acting as a self-regulatory challenge for individuals with high impulsivity or callous-unemotional traits, thereby engaging moral internalization to mitigate these tendencies, as reflected in P300 latency. On the other hand, non-health risk stimuli lack the same morally charged or conflict-laden qualities, failing to provoke similar interactions between intrinsic moral values and attentional processes. The emotionally and morally salient nature of health-risk smoking behavior stimuli likely explains why significant effects were observed only for smoking visuals and why moral internalization, rather than the externally oriented moral symbolization, played a crucial moderating role in these relationships.
The observed finding that only symbolization significantly predicted emotional attention in both the health-risk smoking behavior model and the non-health risk behavior model may be partly explained by the cultural and demographic characteristics of the sample. The sample size was small (N = 21), and the majority of participants were Malay Muslims, which presents a relatively homogenous group in terms of cultural and religious background. In the context of Malay Muslim culture, symbolization, which reflects the degree to which individuals associate moral traits with their self-concept and identity, may be especially salient due to the strong emphasis on moral values, religious teachings, and societal expectations surrounding health and personal conduct. In Islamic teachings, smoking is generally discouraged and increasingly regarded as harmful or even sinful, particularly in Malaysia, where health authorities and religious bodies have jointly advocated against tobacco use. This cultural moral framing could heighten emotional sensitivity to smoking-related cues, particularly among individuals who internalize moral values through symbolic self-representation. Furthermore, emotional attention as indexed by P300-Pz amplitudes may be more strongly activated in individuals who perceive such stimuli as conflicting with deeply held moral or religious norms. This may explain why symbolization-but not traits like narcissism, impulsivity, callous-unemotional traits, or moral internalization-emerged as the only significant predictor in this cultural context. Those other traits, while potentially influential in broader or more diverse populations, may not vary sufficiently within this culturally similar group to show predictive value.
The findings suggest that stigma surrounding smoking-particularly in a Malay Muslim context where smoking is increasingly viewed as morally unacceptable-may underlie the observed neural and psychological patterns. Moral symbolization predicted greater emotional attention to smoking-related and non-health-risk stimuli, suggesting heightened sensitivity to socially disapproved behaviors. This may reflect internal conflict when viewing stigmatized content, especially among individuals who strongly associate morality with their self-concept. The P300 amplitude and latency responses indicate deeper emotional processing and attention allocation to these cues. Additionally, moral internalization controlled the relationship between impulsivity, callous-unemotional traits, and attentional bias, highlighting the moderating role of internalized moral norms. Individuals with low emotional responsiveness may still engage more with stigmatized content when such behaviors violate their internal moral code. These results point to the neurocognitive impact of social stigma, suggesting that culturally embedded moral values shape both behavioral and brain responses to health-risk stimuli like smoking.
5. STUDY LIMITATION
This study has several limitations. First, it focused narrowly on smoking-related visual stimuli, limiting the generalizability of findings to other health or moral domains such as diet, alcohol use, or environmental behavior. The socially charged nature of smoking, especially in cultures where it is stigmatized, may have inflated the role of moral symbolization, which may not hold in less morally salient contexts. Second, potential measurement imbalance between moral symbolization and moral internalization could affect the validity of observed effects. Third, the study emphasized the P300 ERP component without incorporating other relevant markers like N200 or LPP, which could provide a more comprehensive view of emotional and moral processing. Cultural specificity also limits the broader applicability of the findings, as moral interpretations of smoking may vary across societies. Lastly, the absence of behavioral outcome measures restricts conclusions about how neural responses translate into real-world actions, limiting the study’s practical implications for behavior change.
CONCLUSION
This study highlights the distinct roles of moral symbolization and moral internalization in emotional attention processes, particularly in response to smoking-related stimuli. Moral symbolization, focused on external societal norms, significantly predicted attentional biases-as reflected in P300 amplitude-toward both health-risk and non-health risk behaviors. In contrast, moral internalization, representing intrinsic moral values, did not directly predict attentional responses but controlled the relationship between antisocial personality traits and attentional bias, as shown in P300 latency. These findings emphasize the value of combining linear regression and partial correlation to reveal both direct and interactive effects. Theoretically, the study advances understanding of neural mechanisms in moral cognition and self-regulation. Practically, it suggests that public health strategies could leverage moral symbolization in messaging and support internalized moral development to reduce risky behaviors, particularly in individuals with impulsive traits. Future research should validate these findings across diverse populations to broaden their relevance and application.
AUTHORS' CONTRIBUTIONS
The authors confirm contribution to the paper as follows: H.S.K., N.Y.: Study conception and design; N.Y., M.A.A.A.: Data collection; R.S.B., H.S.K.: Analysis and interpretation of results; N.Y., H.S.K.: Draft manuscript. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| ASPD | = Antisocial Personality Disorder |
| ERP | = Event-related Potential |
| EEG | = electroencephalogram |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study protocol received approval from the Universiti Sains Malaysia, Malaysia Human Ethics Committee (approval number: USM/JEPeM/ 19070388).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Participants were given detailed information about the study procedures, and informed consent was obtained from each participant.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
FUNDING
This study was supported by Short-Term Research Grant, Universiti Sains Malaysia – 304/PPSP/6315346
ACKNOWLEDGEMENTS
The author acknowledges the Specialist Hospital Universiti Sains Malaysia.

