All published articles of this journal are available on ScienceDirect.

The Effectiveness of Music Interventions in Exam Anxiety Reduction among University Students –Systematic Review
Authors Info & Affiliations
Abstract
Introduction
Exam anxiety is a common global issue for university students; it is associated with poor academic success and self-confidence. This review investigates the potential benefits of music for reducing anxiety.
Methods
Following the PRISMA guidelines, this review incorporated experimental studies published in English between January 2019 and January 2024, identified through systematic searches of four databases: PubMed, Cochrane Library, ScienceDirect, and Wiley Online Library. Studies meeting the predetermined inclusion criteria underwent methodological quality assessment using the Joanna Briggs Institute (JBI) checklists for randomized controlled trials and quasi-experimental studies.
Results
A review of ten studies, selected from an initial 453, found that music interventions significantly reduced exam anxiety in nine of them. This reduction was evidenced by statistically significant decreases in anxiety scores across various assessment tools (STAI, IEF, VSAF, EAS) and improvements in physiological vital signs.
Discussion
Music interventions are effective in reducing exam anxiety, a non-pharmacological approach that complements existing strategies. This benefit is supported by self-reported and physiological measures, highlighting music's versatility for anxiety management, even in brief applications. It also contributes to student well-being and academic success, aligning with Sustainable Development Goal 3. Further research on music types and individual responses is needed for optimal results.
Conclusion
Exposure to 15 minutes of instrumental classical music before an exam can significantly lower student anxiety. This finding suggests an effective and low-cost way for universities to support student well-being.
1. INTRODUCTION
University life presents a significant and often stressful period, placing considerable pressure on students to achieve academic success [1]. This pressure can lead to student distress, negatively impacting academic performance, increasing dropout rates, and hindering professional development [2]. Anxiety disorders are characterized by excessive worry, nervousness, and unease, frequently out of proportion to any actual threat or occurring without one [3]. While stress is a normal response to demanding situations, prolonged or intense stress can increase the risk of developing anxiety disorders [4]. The interconnected behavioral and neural mechanisms of stress and anxiety indicate that the brain regions and pathways involved in stress response also contribute to the experience of anxiety [5]. Specifically, exam anxiety refers to intense negative emotions and heightened arousal that can manifest before, during, and sometimes after examinations or other forms of assessment [6].
The occurrence of exam anxiety among university students demonstrates considerable variation across different countries. For instance, in Malaysia, around 18% of students reported experiencing test anxiety [7]. However, prevalence rates were notably higher in other regions, with around 33% of students having test anxiety in Saudi Arabia [8]. In Ethiopia, over 52% of medical students reported test anxiety, while nearly 40% of undergraduates in Pakistan experienced moderately high test anxiety [9, 10]. China reported that roughly 34% of students experienced unhealthy test anxiety [11], and in Indonesia, 41% of students preparing for a competency exit exam reported extremely severe exam anxiety [12]. A study comparing UK and US university students (total n=1,776, with a substantial sample from both countries) revealed higher levels of test anxiety among UK students compared to their US counterparts [13]. These diverse findings underscored the widespread presence of exam anxiety, with prevalence rates varying based on geographical location, the specific student population, and the nature of the assessment.
Despite the growing interest in non-pharmacological approaches and the established effectiveness of interventions like cognitive-behavioral therapy and study skills training for exam anxiety, the sustained impact of these methods lacks robust long-term evidence [14]. Research suggested that integrating behavioral or cognitive techniques with skill-focused strategies offers the most promising approach to treating exam anxiety [15]. Various coping programs, music therapy, emotional freedom techniques, animal-assisted intervention, and guided mental imagery have been reported to alleviate test anxiety [16].
However, to fully understand the impact of music interventions on college students' test anxiety, including optimal doses (frequency, duration) and types (e.g., active vs. passive), a targeted systematic review is essential. Furthermore, research might explore effects beyond anxiety reduction, such as on academic performance and physiological stress markers like heart rate and cortisol. This focused investigation would contribute more directly to the evidence-based practice of music interventions.
Music interventions extend across diverse healthcare and social settings [17]. By structuring notes and tones into a cohesive sequence, music generates a continuous experience that promotes emotional, physical, and cognitive well-being through active engagement [18]. As a clinical and evidence-based practice, it pursues specific objectives within the therapeutic relationship [19].
Considerably, listening to calming, slow-tempo music has been shown to reduce anxiety and induce relaxation [20]. This effect is further supported by findings associating music listening with reductions in physiological indicators of anxiety, including blood pressure and heart rate [21], as well as a dampening of the stress response through decreased cortisol levels [22]. The social acceptability, low cost, and ease of integrating music listening into daily routines position it as a practical alternative treatment for anxiety [23]. This underscores the significant potential of music to reduce both physical and psychological stress, with studies indicating its most notable impact on heart rate, followed by reductions in blood pressure and hormone levels [24].
Given the limited systematic evidence available on the effects of music interventions for exam anxiety, particularly regarding doses and types. This review aimed to evaluate the impact of music interventions on reducing exam anxiety among university students. Specifically, to answer the question, how effective is music intervention in reducing exam anxiety in university students? This question was formulated using the Population, Intervention, Comparison, and Outcome (PICO) framework to address the identified gap in the existing literature, as shown in Table 1.
The PICO framework outlined in Table 1 guides the systematic review investigating the effectiveness of music interventions, both alone and in combination with other therapies, for reducing exam anxiety in university students. The population of interest is clearly defined as university students experiencing anxiety specifically related to their examinations. Music can be used alone or in combination with other therapeutic modalities as part of the intervention. Ultimately, the outcome of interest is the reduction in anxiety levels associated with exams, as measured by relevant scales or physiological indicators. This structured approach facilitates a targeted and thorough analysis of the existing research.
| Terms | Meaning |
|---|---|
| Population | University students who are anxious about their exams |
| Intervention | Music intervention OR music intervention combined with other interventions. |
| Comparison | Varies across studies. The review synthesizes comparisons made within the included studies (including comparisons between music alone and music combined with other available interventions). |
| Outcome | Lowering anxiety levels related to exams (measured by a specific scale or multiple scales) |
2. METHODS
A preliminary search of PubMed and the Cochrane Library was conducted to identify systematic reviews on test anxiety in college students before focusing on a specific database. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used to conduct this systematic review [25].
2.1. Databases and Search Strategy
A systematic literature search was conducted using the following keywords to identify articles published between January 2019 and January 2024 in the specified databases. PubMed, ScienceDirect, Cochrane Library, and Wiley Online Library. The KEY (“test anxiety” OR “exam anxiety”) AND (“university students” OR “college students”) AND (“music therapy” OR “music intervention”). In addition to Medical Subject Headings (MeSH) terms. Two reviewers independently reviewed the titles and abstracts of the articles as well as the full-text studies. The PRISMA flow diagram for this systematic review is presented in Fig. (1).
2.2. Eligibility Criteria
The search process focused on interventional studies in university students that aimed to reduce exam anxiety through music interventions. To focus on recent research, the search included English-language publications from January 2019 to January 2024. Additionally, observational studies, articles published in a non-English language, and postgraduate university students, as well as school students, were excluded.
2.3. Quality Assessment
Studies meeting the inclusion criteria underwent methodological quality assessment using the Joanna Briggs Institute (JBI) checklists for randomized controlled trials and quasi-experimental studies [26]. To ensure a thorough evaluation, two independent reviewers, IA and NM, appraised the studies, with any discrepancies resolved through consensus or the involvement of a third reviewer. A comprehensive summary of the risk of bias assessments, including a visual representation across the included studies in Tables 2 and 3.
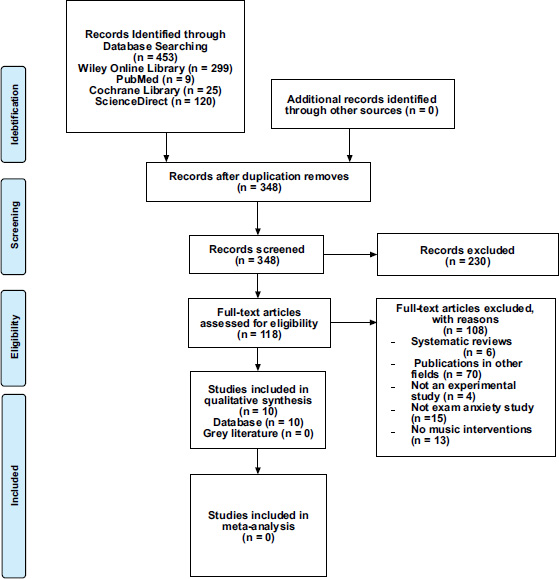
The PRISMA flow diagram for the systematic review.
| Domain | Eyüboğlu et al., 2021 [27] | Inangil et al., 2019 [28] | Song et al.,2019 [29] |
Liu and Li, 2023 [30] |
Inangil et al., 2020 [31] |
Gebhart et al., 2019 [32] | Gllego-Gomez et al., 2020 [33] | Akpinar et al., 2020 [34] |
|---|---|---|---|---|---|---|---|---|
| 1. Was true randomization used for the assignment of participants to treatment groups? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 2. Was allocation to treatment groups concealed? | U | U | Yes | Yes | Yes | Yes | Yes | Yes |
| 3. Were treatment groups similar at the baseline? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 4. Were participants blind to treatment assignment? | No | Yes | Yes | No | Yes | No | No | No |
| 5. Were those delivering treatment blind to treatment assignment? | Yes | U | Yes | Yes | Yes | Yes | Yes | Yes |
| 6. Were outcomes assessors blind to treatment assignment? | Yes | No | Yes | No | No | U | U | Yes |
| 7. Were treatment groups treated identically, other than the intervention of interest? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 8. Was follow-up complete, and if not, were differences between groups in terms of their follow-up adequately described and analysed? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 9. Were participants analysed in the groups to which they were randomized? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 10. Were outcomes measured in the same way for treatment groups? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 11. Were outcomes measured in a reliable way? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 12. Was appropriate statistical analysis used? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 13. Was the trial design appropriate, and were any deviations from the standard RCT design (individual randomization, parallel groups) accounted for in the conduct and analysis of the trial? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Doman | Mojarrab et al., 2020 [35] | Galal et al., 2021 [36] |
|---|---|---|
| 1. Is it clear in the study what the cause is and what the effect is (i.e., there is no confusion about which variable comes first)? | Yes | Yes |
| 2. Were the participants included in any comparison groups? | Yes | Yes |
| 3. Were the participants included in any comparisons receiving similar treatment/care, other than the exposure or intervention of interest? | Yes | Yes |
| 4. Was there a control group? | Yes | No |
| 5. Were there multiple measurements of the outcome, both pre- and post-intervention/exposure? | Yes | Yes |
| 6. Was the follow-up complete, and if not, were differences between groups in terms of their follow-up adequately described and analyzed? | Yes | Yes |
| 7. Were the outcomes of participants included in any comparisons measured in the same way? | Yes | Yes |
| 8. Were outcomes measured reliably? | Yes | Yes |
| 9. Was appropriate statistical analysis used? | Yes | Yes |
2.4. Data Extraction
Two independent reviewers, IA and NM, conducted data extraction using a structured template. The key information retrieved encompassed the authors, study design, participants' major, age, sample size, instruments used, types of interventions implemented, and the outcome of each study, as detailed in Table 4 and Fig. (2), which presents a demographic distribution graph illustrating the publication years and countries of origin for the included studies.
| Authors’/Refs. | Design | Participants' Major | Age | Sample Size | Instruments | Interventions/ Duration | Results |
|---|---|---|---|---|---|---|---|
| Eyuboglu et al., 2021 [27] | RCT/ Quantitative study. | Nursing students. | 18-20 | The 132 participants were allocated to an intervention group (n=61) and a control group (n=64). | The study utilized an informative feature form, STAI, a vital signs assessment form, a skill checklist, and focus group interviews to gather data. | Music therapy, 5 sessions 2/per week for 2 weeks before examinations. A session lasted for 60 minutes. | The average anxiety scores of the control and intervention groups showed no significant difference between the pre- and post-tests (p > 0.05), and students perceived music therapy as a waste of time. |
| Inangil et al., 2019 [28] | RCT | Heath sciences students | 18-22 years | The 90 students in the study were equally distributed across three groups (n = 30 each): Music (Music G), EMT (EMT G), and a control group (CG). | The State-Trait Anxiety Inventory (STAI) was used to evaluate anxiety, and vital signs, specifically blood pressure (BP), pulse, and SpO2, were monitored. | Music intervention for 15 minutes using an MP3 player. Emotional Freedom Technique for 15 minutes, followed by instructions |
Before the intervention, the anxiety levels of the different groups were not statistically significantly different (p = 0.712). However, following the intervention, both the music and EFT groups showed a significant decrease in their average anxiety scores (p < 0.05). |
| Son et al., 2019 [29] | RCT | Female nursing students | 18-24 years | One hundred seven participants were in three groups: Aromatherapy (n=32), music group (n=32), and a combined aromatherapy and music group (n=34). | Anxiety was evaluated using the STAI, stress was measured with a numeric rating score, and a checklist was utilized to assess skill performance. | For 20 minutes leading up to the exam, the Aromatherapy Group inhaled two different essential oils that were diffused into the room. Similarly, the Music Therapy Group listened to “Beethoven Moon Sound” for 20 minutes just before the test. | The combination of aromatherapy and music had a statistically significant impact on reducing exam anxiety (F = 4.77, p = 0.011), and this effect was greater than when music or aromatherapy were used as separate interventions. |
| Liu and Li., 2023 [30] | RCT | Different disciplines | 19-22 years | Two hundred forty participants were equally split into an intervention (n=120) and a control group (n=120). | Zung Self-Rating Anxiety Scale (SAS) | IG received music interventions 3 times a week for 8 weeks. CG received conventional mental health treatment to improve relationships and conflict resolution. |
At the start of the study, there was no statistically significant difference in excessive anxiety levels between the intervention and control groups (p > 0.005). However, college students who participated in music reported a significant reduction in excessive anxiety (p < 0.05). |
| Inangil et al., 2020 [31] | RCT | Nursing students | 18-22 years | Eighty-six participants were recruited and divided into a music group (n=30), an exercise group (n=28), and a control group (CG, n=28). | Anxiety was evaluated using both the state (SAI) and trait (TAI) components. | Music G was applied three times a week for 2 weeks. Exercise G was used for muscle relaxation exercises three times a week for 2 weeks. No intervention was applied to the control group. |
There was no significant difference in the trait anxiety levels between the intervention groups (p>0.05). Music and muscle relaxation exercises can be used to reduce the state anxiety levels in nursing students before the OSCE, p<0.05 |
|
Gebhart et al., 2019 [32] |
RCT | Nursing students | 19-23 years | Seventy-two participants were initially split into three intervention groups and one control group, each with 18 individuals. | Anxiety was measured using the STAI, while levels of the stress hormone cortisol were determined through Saliva ELISA. | Three types of interventions were used: an animal-assisted therapy group, a music group, a mandala painting group, and a control group. Morning interventions (9 AM, 45-60 minutes each) | Focus interventions were associated with a statistically significant reduction in self-reported psychological stress (median: 3.4 cm to 1.1 cm, p < 0.001. Salivary cortisol levels demonstrated a significant decrease (14.2 to 9.7), p < 0.001), while salivary Immunoglobulin A (IgA) levels exhibited a statistically significant increase p <0 .001. |
| Gllego-Gomez et al., 2020 [33] | RCT | Nursing students | 18-30 years. | One hundred twelve participants were equally divided into an intervention group (n=56) and a control group (n=56). | The outcomes assessed in the study were clinical nursing exam scores, blood pressure readings, heart rate measurements, and cortisol levels. | Combination of Progressive Muscle Relaxation (PMR) and music. The intervention for both Progressive Muscle Relaxation (PMR) and music therapy lasted for 1 hour. | The integration of PMR with music therapy can prevent increased cortisol, heart rate, and blood pressure levels. It was also effective in managing and lowering exam-related stress in addition to enhancing academic achievement. |
| Akpinar et al., 2020 [34] | RCT | Several departments | 19-20 years | The 88 participants were divided into an intervention group (n=40) and a control group (n=48). | In addition to assessing examination anxiety with the EAS, the study also measured vital signs. | Classical Western and classical Turkish music 25 minutes 4 days a week for 6 weeks |
On the pretest, the experimental group had an average score of 41.4, with a standard deviation (SD) of 9.4. Following the intervention, the average score decreased to 23.2, and the scores became less spread out (SD of 4.16). Diastolic and systolic blood pressure and pulse rate were lower among students who listened to music. |
| Mojarrab et al.,2020 [35] | Quasi-experimental design | Nursing students | 20-25 years | The 76 participants were divided into an intervention group (n=41) and a control group (n=35). | Anxiety was assessed using the State-Trait Anxiety Inventory (STAI). | The intervention group received a 40-minute Coping program three times weekly on exam eve, integrating muscle relaxation, diaphragmatic breathing, and instrumental music. | Following the clinical examination (OSCE), there was a significant difference in pre-/post- scorers between the control and intervention groups, p<0.001. Anxiety coping program reduces the anxiety by 11.61 units in the IG. |
| Galal et al., 2021 [36] | Quasi-experimental design | Pharmacy students | 18-23 years | A total of 202 participants were included in the study, distributed between two experimental groups, with 103 participants in the first group and 99 in the second group. | (STAI) | Active music playing versus Passive music listening. Self-selected music for 25 minutes or played percussive instruments for 25 minutes. |
The study concluded that even a single brief music session was effective in reducing test anxiety, regardless of whether students listened passively or actively engaged in playing. Notably, anxiety levels rose in anticipation of the test before the music intervention and then declined afterward for both listening and playing groups. |
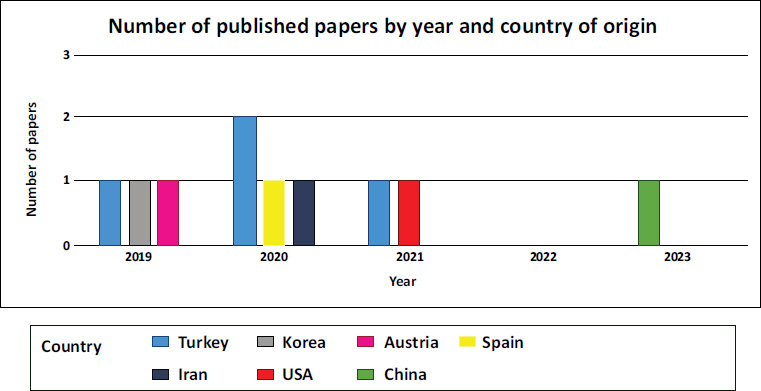
A demographic distribution graph showing the publication years and countries of origin for the included studies.
3. RESULTS
3.1. Study Selection
The initial search across the four databases yielded 453 studies. Of these, 335 were excluded. One hundred and five due to being duplicate records, and 230 for other reasons, such as incomplete full-text articles, publication before 2019, or being in a language other than English. Following the screening of 118 studies, a further 108 were excluded for reasons including being systematic reviews, publication in unrelated fields, not employing RCT or quasi-experimental designs, not focusing on test anxiety, and lacking music interventions. The management of downloaded citations from the databases was facilitated by Zotero, which enabled the identification and removal of duplicate records. Ultimately, ten studies met the inclusion criteria and were included in this review. The flow diagram illustrating the study selection process is presented in Fig. (1).
3.2. Summary of Included Studies
The review included ten studies from seven different nations. The total sample size across these studies was 1205 university students. The largest sample size was n = 240 in a study from China [30], while the smallest was n = 72 in a study from Austria [32]. There were four studies from Turkey [27, 28, 31, 34], one from Korea [29], one from China [30], one from Iran [35], one from Austria [32], one from Spain [33], and one from the United States [36]. Two of the studies utilized quasi-experimental designs [35, 36], seven used RCTs [28-34], and one was a mixed-methods study that employed both RCTs and convergent parallel analysis [27]. One of the two quasi-experimental studies lacked a control group, and not all RCT studies employed a double-blind approach, which introduces a potential source of bias. As shown in Table 4 and Fig. (2).
Regarding the participants' academic backgrounds, the review revealed a significant focus on nursing, as seven of the ten included studies specifically examined nursing students. The other three investigations involved more diverse groups, including health sciences students, individuals from various academic fields, and pharmacy students [30, 34, 36].
Nine of the ten studies in this collection included both male and female participants, indicating that the participant demographics were generally inclusive of both genders. Female participants were the only subjects of one research study [29]. The average participant age across the 10 studies was 21.05 years.
The ten studies employed various instruments to collect data, with a strong emphasis on assessing anxiety. The State-Trait Anxiety Inventory (STAI) was the most frequently used tool, appearing in six studies [27-29, 32, 35, 36]. Several studies also incorporated physiological measures, such as vital signs (blood pressure, pulse, SpO2) and cortisol levels (measured via Saliva ELISA), to assess physiological responses related to anxiety and stress [27, 28, 32-34]. Additionally, one study utilized an informative feature form, a skill checklist, and focus group interviews [27], while another employed a numeric rating scale for stress and a skill performance checklist [29], and the Zung Self-Rating Anxiety Scale (SAS) was specifically used to assess anxiety in one study [30].
The overall duration of these interventions varied considerably, ranging from single sessions in studies [28, 29, 33] to multi-week programs with different session frequencies. Examples include five sessions over two weeks [27], three sessions per week for eight weeks [30], three sessions per week for two weeks [31], four days a week for six weeks [34], and three sessions per week on the evening before an exam [35]. The length of individual sessions also differed significantly, from 15 minutes [28] to 60 minutes [27].
Furthermore, some studies specified the type of music used, such as “Beethoven moon sound” [29], relaxing music [33], classical Western and classical Turkish music [34], and self-selected music [36], while others provided less detail. The method of music delivery also varied, including MP3 players [28], diffused music [29], CD players without headphones [33], and even active participation by playing percussive instruments versus passive listening through headphones [36], as shown in Table 4.
3.3. The Effectiveness of Music Interventions
The purpose of the ten investigations was to find out whether music could help university students who were severely anxious or anxious about exams. Across the ten studies, nine demonstrate that music consistently emerged as a beneficial intervention for reducing anxiety in various settings [28-36]. Multiple studies demonstrated its effectiveness as a standalone treatment, leading to significant decreases in self-reported anxiety levels, whether general, exam-related, or situational, like pre-OSCE state anxiety [28, 30, 31, 36].
Interestingly, the positive impact of music intervention was amplified when combined with other approaches such as aromatherapy [29] and progressive muscle relaxation [33], suggesting a synergistic effect. Beyond subjective reports, physiological benefits were also observed, with music associated with lower blood pressure and pulse rate [34] and a prevention of stress-induced cortisol increases [33, 34]. One study indicated a broader impact on psychological stress and immune markers [32], although the specific role of music within that “focus intervention” is not solely isolated. Notably, even brief music interventions, whether through passive listening or active engagement, proved effective in alleviating test anxiety [36], particularly by counteracting the anticipatory rise in anxiety before an exam. When compared to other techniques like muscle relaxation, music demonstrated comparable efficacy in reducing anxiety [31]. Importantly, the initial similarity in anxiety levels across different groups before the interventions strengthens the conclusion that the subsequent reductions were attributable to the music intervention itself [28, 30].
4. DISCUSSION
The study employs a narrative synthesis methodology, avoiding quantitative evaluation due to clinical and methodological variability. This heterogeneity is due to diverse data collection instruments, intervention durations, and music types. The narrative discusses variations in study design, population characteristics, interventions, outcome measures, and delivery methods.
The majority of studies reviewed consistently demonstrate music's effectiveness in reducing anxiety across various contexts, with nine out of ten showing a significant anxiety-reducing effect either alone or combined with other approaches [28-36]. While one study noted improved blood pressure without affecting anxiety or exam performance, suggesting a need for more sessions or varied student groups [27], the overall findings are compelling. This consistent impact is particularly noteworthy given the significant methodological and clinical heterogeneity among the included music interventions. As detailed, studies varied widely in duration, specific music types, and delivery methods (e.g., from single 15-minute passive listening sessions to multi-week active programs). This broad applicability indicates that music's anxiety-reducing benefits are not confined to a narrow set of parameters, offering flexible and practical applications, akin to other established strategies such as systematic desensitization, exercise, hypnotherapy, relaxation training, and CBT [14, 16].
This benefit was observed not only in self-reported anxiety levels but also in physiological markers of stress, such as blood pressure, heart rate, and cortisol levels, indicating a comprehensive impact on the stress response system. The synergistic effects observed when music was combined with aromatherapy and progressive muscle relaxation highlight the potential for multimodal approaches to anxiety management [29, 33]. Furthermore, the effectiveness of even brief music interventions in alleviating acute stressors such as exam anxiety underscores their practicality and accessibility in time-sensitive situations. While the evidence overwhelmingly supports the anxiety-reducing effects of music therapy, it is important to acknowledge the nuances within the findings. The “focus intervention” study [32] suggests a broader impact on psychological stress and immune markers, but the specific contribution of music within this multifaceted intervention remains unclear.
The analyzed music intervention studies [27, 36] demonstrate significant variability in intervention protocols, encompassing differences in overall duration (from single sessions, as seen in studies [28, 29, 33], to multi-week programs), session length (ranging from 15 minutes [28] to 60 minutes [27]), specific music genres (including, for instance, “Beethoven moon sound” [29] or self-selected music [36]), and delivery methods, such as MP3 players [28] or group listening [33].
This lack of standardization in music intervention protocols likely stems from diverse research aims and varying hypotheses about optimal dosage and engagement strategies to achieve outcomes like immediate anxiety reduction or sustained well-being. To enhance the interpretability and precision of these findings, the narrative synthesis allowed for a deeper exploration into whether shorter versus longer interventions yield different levels of effectiveness, if specific populations are more responsive, and which delivery methods produce stronger effects.
Music listening has a significantly large overall effect on alleviating anxiety and appears to be a cost-effective way to improve student well-being [37, 38]. Music interventions and Emotional Freedom Techniques (EFT) offer accessible and safe methods for potentially reducing exam anxiety and enhancing performance in university students [28]. However, the impact of music on emotions is indeed complex. It is known that the strength of both positive and negative affect depends on the type of musical influence and the baseline neurochemical state. In particular, the perception of the same music can be rated positively at one phase of the women's cycle and negatively at another [39, 40]. This variation, together with the impact of age, emphasizes the need for care when concluding the beneficial effects of music for anxiety.
Directly contributes to Sustainable Development Goals (SDGs) 3 (Good Health and Well-being) and 4 (Quality Education). By offering accessible and engaging interventions, music can address prevalent issues like stress, anxiety, and depression among university students, fostering improved mental health and emotional regulation [41]. This aligns with SDG 3 by promoting overall well-being and reducing the burden of mental health challenges.
Furthermore, by creating a more supportive and emotionally balanced learning environment, music can indirectly enhance students' concentration, focus, and academic performance [42, 43]. Thus contributing to the aims of SDG 4, which emphasizes quality education and the creation ofeffective learning environments. Integrating music into school settings can be a financially sound strategy, especially when compared to more resource-intensive interventions, offering a scalable and sustainable way to support student well-being and facilitate their educational success.
Numerous constraints exist within the investigations. For example, few studies focused on first- or second-year students from a single university [33, 36] or employed convenience sampling [27], and some focused on female participants [29]. This narrow focus, sometimes restricted to specific departments [34], sometimes extrapolates results to broader student populations or different academic disciplines. Additionally, factors such as the short duration of interventions [27, 35], potential power imbalances between researchers and participants [27], the reliance on self-report measures without physiological validation [29], the possibility of a placebo effect [29], small intervention group sizes [32], and the lack of longitudinal follow-up to assess the sustained effects of interventions were noted across the ten studies.
Moreover, the JBI quality assessment highlighted inconsistencies in blinding across the included studies, potentially affecting the conclusions. Only three out of eight relevant studies [28, 29, 31] successfully blinded participants. This lack of blinding in the remaining five studies introduces the risk of performance and detection bias. Specifically, participants' awareness of receiving music therapy could lead to an expectation of reduced anxiety, potentially inflating the observed treatment effect in these studies (Supplementary Material).
4.1. Implications
Over the last decade, research into how the brain responds to emotions triggered by music has greatly improved our understanding of human feelings [44]. Studies using functional brain imaging show that music can change activity in brain areas known to be critical for emotion, such as the amygdala, hypothalamus, hippocampus, insula, and orbitofrontal cortex [44-46]. The finding that calming music significantly reduced self-reported anxiety aligns with CBT principles by demonstrating a reduction in physiological arousal often associated with anxious thought patterns, suggesting music can be a direct intervention for the somatic symptoms of anxiety [24].
Beyond CBT, the Social Cognitive Theory (SCT) sees music as an active environmental influence. Through direct “mastery experiences,” when people effectively utilize music to reduce anxiety, it can increase self-efficacy by reaffirming their conviction in their coping mechanisms [47, 48]. It is noteworthy that listening to music can raise scores on resilience, optimism, self-efficacy, purpose in life, and psychosocial well-being [49, 50].
4.2. Limitations and Future Research
This review examines the impact of music interventions on exam anxiety in university students, offering potential strategies for administrators, students, mental health professionals, and parents. However, limitations include the limited number of English-published studies, heterogeneity in outcome assessment tools, and potential bias in the double-blind methodology.
Future research on music interventions should consider diverse student populations, cultural backgrounds, academic disciplines, and initial levels of anxiety. Longitudinal studies with follow-up assessments are crucial for ensuring long-term sustainability. Large-scale randomized controlled trials and subsequent follow-up evaluations will provide a more robust evidence base.
CONCLUSION
The narrative synthesis, encompassing diverse methodologies and music interventions, consistently demonstrates that music effectively reduces anxiety, including exam anxiety, in university students. This benefit extends beyond self-reported measures to physiological markers of stress, underscoring music's potential as a versatile, accessible, and cost-effective non-pharmacological strategy for mental well-being.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: I.A.: Responsible for conceptualization, investigation, critical appraisal, search strategy, writing, and editing; N.M.: Responsible for developing the research question and conducting the literature search, writing, and editing; M.A.: Responsible for developing the research question and conducting the literature search; P.P.: Contributed to the investigation, validation, writing, and editing; H.A.: Contributed to the quality assessment, writing, and editing; E.J.: Contributed to the quality assessment, writing, and editing. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| PRISMA | = Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| OSCE | = Objective Structured Clinical Examination |
| JBI | = Joanna Briggs Institute checklists |
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article will be available from the corresponding author [I.A] upon reasonable request.
ACKNOWLEDGEMENTS
Declared none.

