All published articles of this journal are available on ScienceDirect.

Psychometric Evaluation of the Malay Version of the Mental Health Knowledge Schedule (MAKS-M): Evidence of Structural and Cultural Limitations
Authors Info & Affiliations
Abstract
Introduction
Mental health literacy instruments are often adapted across cultures with the assumption that their constructs remain stable. This study critically evaluates the psychometric performance of the Malay version of the Mental Health Knowledge Schedule (MAKS-M) to examine whether its original structure transfers to the Malaysian context and to identify factors contributing to cross-cultural underperformance.
Methods
A cross-sectional survey was conducted among 203 university-based respondents. Reliability indices, confirmatory factor analysis (CFA), and convergent validity testing were used to assess structural performance.
Results
Both subscales showed poor internal consistency (knowledge: α = 0.262; attitude: α = 0.236) and weak item-rest correlations, with reversed items performing particularly poorly. CFA indicated suboptimal model fit (CFI = 0.712, RMSEA = 0.124), with several reversed items showing non-significant or negative factor loadings. Convergent validity was partially supported through significant correlations with the BIPM interest subscale.
Discussion
The MAKS-M demonstrated significant psychometric limitations, likely due to linguistic ambiguities, cultural incongruities, and conceptual overlap between knowledge and attitude constructs. In particular, reversed items appear especially vulnerable to linguistic and cultural misinterpretation, and the results suggest that the MAKS factor structure may not be inherently stable when applied outside Western sociocultural contexts.
Conclusion
Rather than confirming validity, the study identifies structural and cultural barriers to the reliable use of the MAKS in Malaysia. The findings highlight broader methodological challenges in direct cross-cultural scale adaptation.
1. INTRODUCTION
Mental health literacy refers to the knowledge and beliefs concerning mental disorders that facilitate their identification, management, or prevention [1]. It is a crucial factor in reducing stigma and encouraging timely help-seeking behaviors [2]. Evaluating the public’s understanding of and attitudes toward mental health is therefore fundamental to the development of effective educational initiatives and anti-stigma interventions [3]. The Mental Health Knowledge Schedule (MAKS), created by Evans-Lacko and colleagues (2010), is a concise self-report tool designed to measure two main aspects of mental health literacy: objective knowledge and stigma-related attitudes [4].
Although the MAKS has been used in various countries, its application outside English-speaking contexts requires careful translation and cultural adaptation [5, 6]. Cross-cultural validation is vital because cultural norms [7], language nuances [8], and conceptualizations of mental health [9] can influence how respondents interpret scale items, potentially affecting measurement reliability and validity [10]. In Malaysia, mental health literacy research is growing, but there remains a lack of rigorously validated Malay-language tools for measuring both knowledge of and attitudes toward mental health [11, 12]. Mental health literacy is not a purely cognitive construct in the Malaysian context; interpretations are shaped by cultural norms, moral beliefs, and religious meaning systems. As such, instruments developed in Western settings require conceptual adaptation, not solely translation.
The MAKS consists of 12 items: six assessing knowledge of mental health-related facts and conditions and six assessing stigma-related attitudes toward mental health [4]. Its brevity and ease of administration make it attractive for large-scale surveys, but concerns have been raised regarding the performance of certain items-particularly reversed items-which have been shown to introduce response biases and reduce internal consistency [12].
Previous validation studies have yielded mixed results. For example, studies in European settings have generally supported the two-factor structure but reported modest internal consistency, especially for the knowledge subscale [4]. Research in Asian contexts, such as China and Singapore, has highlighted additional challenges: linguistic translation may alter item meaning, reversed items may cause confusion, and ceiling effects may occur in populations with high baseline familiarity with mental health topics [13, 14].
In Malaysia, few instruments have been validated for the simultaneous assessment of mental health knowledge and stigma-related attitudes. Existing studies have often relied on unvalidated or partially adapted tools, limiting the comparability and interpretability of findings [15, 16]. A validated Malay version of the MAKS could fill this gap, enabling consistent measurement across research, policy evaluation, and community education initiatives. However, any adaptation must be rigorously tested to ensure that it maintains conceptual equivalence, cultural relevance, and robust psychometric properties [6, 17, 18].
Despite the widespread use of mental health literacy instruments across cultural contexts, most validation studies implicitly assume that the underlying constructs and factor structures of the original scales are stable and transferable [17]. Consequently, cross-cultural adaptations often focus on improving model fit or internal consistency rather than explicitly testing whether the original construct architecture remains valid in non-Western settings. When instruments such as the MAKS are adopted uncritically, there is a risk that observed scores may reflect measurement artefacts rather than true differences in mental health knowledge or stigma-related attitudes, potentially leading to misleading research conclusions and policy decisions [17, 18].
Accordingly, the present study is not positioned as a conventional validation exercise aimed at endorsing the MAKS-M for applied use. Instead, it is framed as a critical psychometric evaluation that examines whether the theoretical structure, item design, and measurement assumptions of the original MAKS remain valid when transferred to a Malaysian cultural and linguistic context. By documenting points of psychometric failure rather than obscuring them, this study contributes methodological insight into the limits of direct scale adaptation in cross-cultural mental health research.
2. METHODOLOGY
This research focuses on the translation, cultural adaptation, and validation of the Mental Health Knowledge Schedule (MAKS-M) for application among Malay-speaking individuals in Malaysia. Standardized international guidelines for cross-cultural adaptation were followed, after which several psychometric evaluations were conducted to assess the scale’s reliability and construct validity [18]. An overview of the study process is presented in the flowchart (Fig. 1).
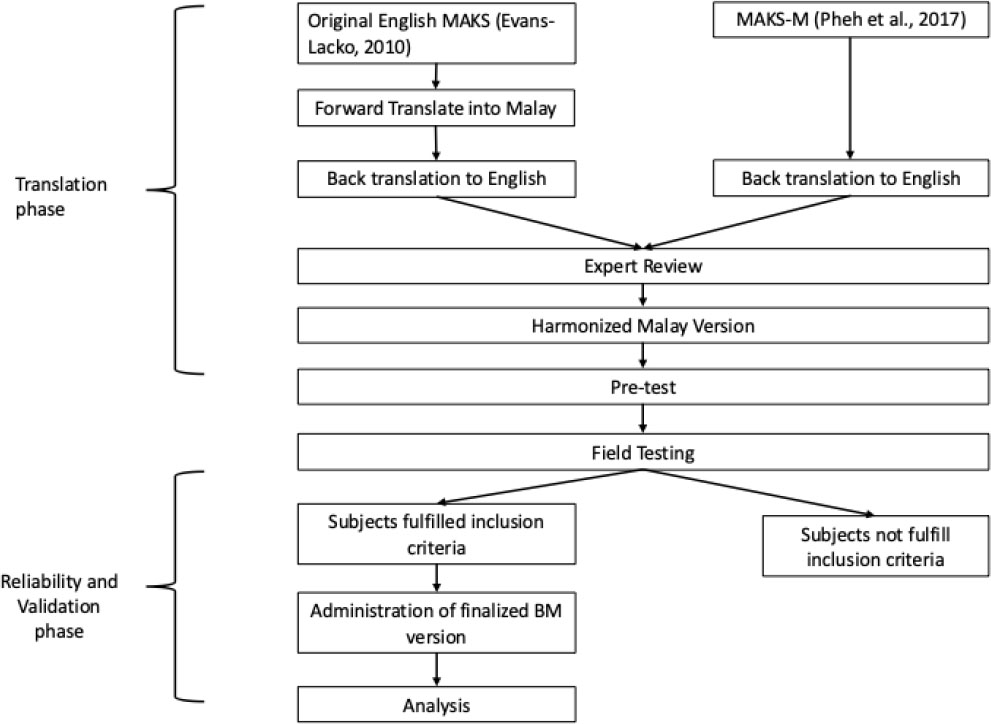
Translation and validation flowchart.
2.1. Translation Process
The translation process involved both the original English version and the previously tested MAKS-M by Pheh et al. (2017) [19].
The original MAKS, developed in English, was translated into Malay following a standardized forward-backward translation procedure based on WHO guidelines. A bilingual expert independently forward-translated the scale into Malay. A separate bilingual translator, blinded to the original version, then back-translated the Malay version into English.
The Mental Health Knowledge Schedule-Malay Version (MAKS-M) is an adapted version of the original 12-item MAKS that was previously translated and underwent preliminary validation by Pheh et al. (2017) [19]. The MAKS-M was further evaluated by having another team of translators back-translate it into English.
Both versions were compared and reviewed by a panel of three experts in both the linguistic and clinical fields. During the review, some minor changes were made to the language for better clarity, such as the addition of descriptions to Item 10, “bipolar disorder” (English version), and Item 12, “grief” (English version), by providing direct Malay translations with descriptions for better clarity. The word “problems” in the translation was also replaced with “symptoms” in Malay to reduce stigma in language delivery. The overall context and structure of the scale remained unchanged.
The final translated version is shown in Appendices A and B.
2.2. Pre-test and Field Testing Process
A preliminary test with 20 bilingual university students was carried out to evaluate the face validity and clarity of the translated MAKS items. Feedback from this group led to minor linguistic revisions that enhanced the readability of the Malay version. These individuals were excluded from the main validation sample, and their responses were used solely for refinement before broader field testing.
For field testing, a cross-sectional study design was adopted to examine the psychometric characteristics of the Malay Mental Health Knowledge Schedule (MAKS-M). Data were obtained from 203 participants enrolled at a public university in Malaysia and recruited through convenience sampling between 1 June 2025 and 10 August 2025. Participants received study information and provided informed consent before completing the questionnaires. No personal identifiers were collected, and once submitted, responses could not be altered or resubmitted.
Respondents first completed the Malay version of the MAKS, followed by the Balanced Index of Psychological Mindedness (BIPM), and finally the original English version of the MAKS. The recruitment of bilingual students ensured language proficiency and familiarity with self-administered questionnaires, allowing for reliable comparisons between the Malay and English versions. This procedure is consistent with common practices in preliminary validation research designed to assess psychometric performance [6].
While this design allows for a preliminary assessment of conceptual equivalence, it may also introduce priming or contamination effects, whereby exposure to one language version influences responses to the other. Accordingly, bilingual administration may be acknowledged as a methodological limitation rather than a strength, and the findings should be interpreted with caution.
2.3. Inclusion and Exclusion Criteria
Inclusion criteria for participation were as follows: (i) aged 18 years and above; (ii) literate in both Malay and English; (iii) currently enrolled as university students; (iv) no reported history of major psychiatric or neurological disorders (self-declared); and (v) provided informed consent to participate in the study.
Participants were excluded if they: (i) had insufficient proficiency in either Malay or English to complete the study questionnaires reliably; (ii) reported a current or past diagnosis of a severe psychiatric disorder (e.g., psychosis, bipolar disorder) that could impair comprehension or participation; or (iii) had previously participated in the pilot/face validity testing phase of this study.
All participants were non-clinical volunteers.
2.4. Sample Size
Sample size determination was guided by established psychometric guidelines for validation studies. A minimum subject-to-item ratio of 10:1 was set to ensure adequate statistical power for internal consistency analysis and confirmatory factor analysis (CFA), as recommended in scale development literature [20, 21]. Additionally, a medium effect size (Cohen’s d = 0.5), which is widely accepted as the minimum threshold for significance in psychometric research, was used as a benchmark for sample adequacy.
The Malay version of the Mental Health Knowledge Schedule (MAKS-M) comprises 12 items divided into two subscales: (i) Subscale A (Mental Health Knowledge): 6 items; (ii) Subscale B (Stigma-related Attitudes): 6 items.
Based on the minimum ratio of 10 participants per item, the required sample size was calculated as:
Required minimum sample size = Number of items × 10 = 12 × 10 = 120 participants
A total of 203 participants were successfully recruited, which exceeds the recommended minimum and provides a stable basis for evaluating internal consistency (e.g., Cronbach’s α, McDonald’s ω), item-total correlations, and the factorial structure through CFA. This sample size also ensures sufficient power for testing convergent validity with related constructs such as psychological mindedness [20].
2.5. Measurements
2.5.1. Mental Health Knowledge Schedule (MAKS)
The Mental Health Knowledge Schedule (MAKS) is a validated instrument developed by Evans-Lacko et al. (2010) to assess stigma-related knowledge about mental health among the general public. It was designed to address the lack of psychometrically sound tools for evaluating mental health literacy, particularly within the context of stigma-reduction interventions [4].
The MAKS consists of 12 items divided into two main sections: Items 1 to 6 assess general stigma-related knowledge across six domains: help-seeking, recognition, support, employment, treatment, and recovery; Items 7 to 12 evaluate participants’ recognition of specific conditions (e.g., depression, schizophrenia) as mental health problems, providing context for interpreting conceptualizations of mental illness.
Respondents rate their agreement with each statement on a 5-point Likert scale ranging from strongly disagree (1) to strongly agree (5), with an option for “don’t know” coded as neutral (3). Several items are reverse-scored to reflect correct knowledge direction.
Psychometric evaluation demonstrated that the MAKS has moderate internal consistency (Cronbach’s α = 0.65 for items 1-6) and good test-retest reliability (Lin’s concordance coefficient = 0.71), with individual item kappa values ranging from 0.57 to 0.87. While the tool was not designed to function as a unidimensional scale, it captures diverse knowledge components relevant to stigma, making it suitable for item-level analysis [4].
2.5.2. Balanced Index of Psychological Mindedness - Malay Version (BIPM-M)
The BIPM-M is a 14-item self-report instrument adapted from the original BIPM to assess individuals’ insight and interest in psychological processes. The scale was translated into Bahasa Malaysia following WHO guidelines, involving forward- and backward-translation by language and content experts, followed by pre-testing with 50 native speakers. A cross-sectional validation study involving 141 university students was conducted to evaluate its psychometric properties [22].
Factor analysis confirmed a two-factor structure (Insight and Interest), consistent with the original scale. The BIPM-M demonstrated excellent internal consistency (Cronbach’s α = 0.87) and strong reliability (McDonald’s ω = 0.88; GLB = 0.95). It showed moderate correlations with AAQ-II and MAAS, supporting its concurrent validity. The BIPM-M is a culturally appropriate and psychometrically sound tool for measuring psychological mindedness among Malay-speaking populations [22].
2.6. Data Analysis Methods
The data analysis to validate the Malay version of the Mental Health Knowledge Schedule (MAKS-M) was conducted systematically to establish the instrument's reliability and validity. To begin, internal consistency was assessed using Cronbach’s alpha, which evaluates the degree to which items within a scale are interrelated [23]. Each of the two subscales-Mental Health Knowledge (items 1 to 6) and Stigma-related Attitudes (items 7 to 12)-was analyzed independently to ensure that the translated items consistently measured their respective constructs. Higher Cronbach’s alpha values indicate greater internal consistency, with values above 0.70 generally considered acceptable [23].
In addition to Cronbach’s alpha, McDonald’s omega and the Greatest Lower Bound (GLB) reliability coefficients were computed for both subscales. McDonald’s omega accounts for varying factor loadings across items, offering a more precise estimate of reliability in cases where the assumption of equal item contribution (tau-equivalence) may not be met [24]. GLB, on the other hand, provides a lower-bound estimate of true reliability and is especially useful in psychometric evaluations when item true-score variances differ. A GLB value exceeding 0.80 is typically indicative of strong internal consistency and adds further confidence in the scale’s reliability. Corrected item-total correlations, often referred to as item-rest correlations, were computed to evaluate reliability at the item level. This statistic indicates the relationship between a single item and the total score of the remaining items within the subscale, thereby showing the extent to which each item corresponds to the construct being measured [24].
Construct validity was assessed by examining both convergent and discriminant validity. Convergent validity was evaluated by computing Spearman’s correlation coefficients between the MAKS-M subscales and the subscales of the Balanced Index of Psychological Mindedness (BIPM), namely Interest and Insight. These constructs are theoretically related to mental health knowledge and openness to psychological understanding, and moderate to high positive correlations were expected. Discriminant validity was determined by comparing correlations between the MAKS-M and constructs assumed to be theoretically unrelated. This approach allowed for an evaluation of the scale’s ability to differentiate between related and unrelated constructs. The use of Spearman’s rho was justified due to the non-normal distribution of the subscale scores, as indicated by both the Kolmogorov-Smirnov and Shapiro-Wilk tests.
To further examine cross-language construct equivalence, a subset of bilingual participants completed both the English and Malay versions of the MAKS. Spearman correlations were calculated between subscale scores across the two versions. High correlation coefficients would suggest that the translated version retains conceptual and measurement equivalence with the original English scale, thereby supporting its use in the local context [25, 26].
Confirmatory factor analysis (CFA) was conducted to test the transportability of the original two-factor structure proposed by Evans-Lacko et al., rather than to optimise model fit within the Malaysian sample. As the dimensionality of the MAKS is theoretically predefined, a theory-driven confirmatory approach was prioritised to evaluate structural equivalence before considering exploratory alternatives.
Confirmatory factor analysis was conducted using maximum likelihood estimation to allow comparison with the original MAKS validation framework. However, given the clear evidence of non-normal item distributions, the use of maximum likelihood (ML) estimation may have resulted in conservative or unstable fit indices. As such, CFA findings are interpreted primarily as diagnostic indicators of structural viability rather than confirmatory tests of model adequacy. Factor loadings for individual items were inspected to determine their contribution to the respective constructs, with values above 0.40 regarded as satisfactory indicators [24, 27].
The adequacy of the model was judged through multiple fit indices, including the Comparative Fit Index (CFI), Tucker-Lewis Index (TLI), Root Mean Square Error of Approximation (RMSEA), and Standardized Root Mean Square Residual (SRMR). Criteria for acceptable model fit required CFI and TLI values greater than 0.90, RMSEA below 0.08, and SRMR below 0.08 [27, 28]. Collectively, these indices provided a robust appraisal of how well the hypothesized two-factor structure aligned with the observed data, thereby reinforcing the scale’s structural validity.
3. RESULTS
The study involved 203 respondents with a mean age of 26 years, with the majority (70.4%) being under 25 years old. Most participants were female (68.0%), and the predominant education level was a bachelor’s degree (74.9%), with smaller proportions holding a master’s degree (7.4%), diploma (6.9%), secondary school education (8.4%), DrPH (2.0%), or primary school education (0.5%). In terms of occupation, nearly three-quarters (72.9%) were students, followed by employed individuals (20.2%), unemployed participants (6.4%), and one retiree (0.5%). A large proportion of respondents (81.3%) reported that they currently know or have known someone with a mental health problem, indicating high familiarity with the topic (Table 1).
| - | - | Mean | Count | Column N % |
|---|---|---|---|---|
| Age (years) | - | 26 | - | - |
| Age group | Less 25 years old | - | 143 | 70.4% |
| 25 years old and above | - | 60 | 29.6% | |
| Gender | Male | - | 65 | 32.0% |
| Female | - | 138 | 68.0% | |
| Education level | Primary school | - | 1 | 0.5% |
| Secondary school | - | 17 | 8.4% | |
| Diploma | - | 14 | 6.9% | |
| Bachelor's degree | - | 152 | 74.9% | |
| Master's degree | - | 15 | 7.4% | |
| DrPH | - | 4 | 2.0% | |
| Occupation status | Student | - | 148 | 72.9% |
| Employed | - | 41 | 20.2% | |
| Unemployed | - | 13 | 6.4% | |
| Retiree | - | 1 | 0.5% | |
| Known, or have known, someone with a mental health problem | Yes | - | 165 | 81.3% |
| No | - | 38 | 18.7% |
3.1. Descriptive Analysis
Table 2 presents descriptive analyses of the 12 items of the Malay version of the Mental Health Knowledge Schedule (MAKS-M), with mean scores ranging from 2.764 (Item 8, reversed “Stress [English ver.]”) to 4.650 (Item 10, “Bipolar Disorder (manic-depression)[English ver.]”). Items from the knowledge subscale (Items 1-6, with Item 6 reversed) generally scored between 2.837 and 4.187, with skewness values mostly negative except for the reversed items. Items from the attitude subscale (Items 7-12, with Items 8 and 12 reversed) showed means from 2.764 to 4.650, with several items (e.g., Items 7 “Depression [English ver.]”, 9 “Schizophrenia [English ver.], and 10 “Bipolar Disorder (manic-depression)[English ver.]”) displaying strong negative skewness. Kurtosis values varied, with some high positive values (e.g., Item 9 = 3.158), particularly for items with extreme skewness. The minimum and maximum scores covered the full range (1-5; Appendix C).
| Subscale | Number of Items | Mean (SD) | Observed Range | Skewness Range | Kurtosis Range |
|---|---|---|---|---|---|
| Knowledge (Items 1-6*) | 6 | 3.68 (0.62) | 2.17 - 4.60 | -0.73 to +0.08 | -0.90 to +0.64 |
| Attitude (Items 7-12*) | 6 | 3.93 (0.79) | 1.17 - 4.93 | -1.86 to +0.10 | -1.11 to +3.16 |
Notes: * Items 6, 8, and 12 are reversed items included in the total subscale scores.
Full item-level descriptive statistics are presented in Appendix C.
The normality tests for the MAKS-M subscales indicated that both the knowledge (sum of Items 1-6, with Item 6 reversed) and attitude (sum of Items 7-12, with Items 8 and 12 reversed) scores deviated significantly from normality. For the knowledge subscale, the Kolmogorov-Smirnov test (D = 0.109, p < .001) and the Shapiro-Wilk test (W = 0.979, p = .004) both yielded significant results, suggesting non-normality. Similarly, for the attitude subscale, the Kolmogorov-Smirnov test (D = 0.135, p < .001) and the Shapiro-Wilk test (W = 0.959, p < .001) confirmed a significant departure from normality (Table 2).
3.2. Reliability Analysis
The reliability analysis of the MAKS-M subscales showed poor internal consistency in both the knowledge and attitude domains. For the knowledge subscale (Items 1-6, with Item 6 reversed), McDonald’s ω was 0.396, Cronbach’s α was 0.262, and the Greatest Lower Bound (GLB) was 0.480, with the 95% confidence intervals (Table 3). Notably, Item 6 (reversed) “Most people with mental health problems… [English ver.]” correlated negatively with the overall scale (Appendix D) [25].
| Subscale | McDonald’s ω | Cronbach’s α | GLB | α (after removing reversed items) | Interpretation |
|---|---|---|---|---|---|
| Knowledge | 0.396 | 0.262 | 0.480 | 0.500 | Poor reliability |
| Attitude | 0.444 | 0.236 | 0.646 | 0.566 | Poor reliability |
Notes: - GLB: Greatest Lower Bound.
-Removal of reversed items (Items 6, 8, and 12) improves internal consistency but remains below acceptable thresholds (α ≥ 0.70).
-Full reliability diagnostics are presented in Appendix D.
Similarly, for the attitude subscale (Items 7-12, with Items 8 and 12 reversed), McDonald’s ω was 0.444, Cronbach’s α was 0.236, and the GLB was 0.646. Item 8 (reversed), “Stress [Eng ver.]”, also showed a negative correlation with the scale.
The item-level reliability analysis for the MAKS-M knowledge subscale (Items 1-6, with Item 6 reversed) showed that most items had low item-rest correlations. Item-rest correlations ranged from 0.046 (Item 5) to 0.413 (Item 4). Notably, Item 6 (reversed), “Most people with mental health problems… [English ver.],” had a negative item-rest correlation (-0.200). Cronbach’s α values if an item was deleted showed that removing Item 6 would substantially increase α from 0.262 to 0.500.
The item-level reliability analysis for the MAKS-M attitude subscale (Items 7-12, with Items 8 and 12 reversed) revealed notable variability in item performance. Most items showed moderate positive item-rest correlations (0.259 to 0.555), with Items 9, “Schizophrenia [Eng ver.]”, and 10, “Bipolar Disorder (manic-depression) [Eng ver.],” having the highest correlations (0.524 and 0.555, respectively). In contrast, Item 8 (reversed), “Stress [Eng ver.],” and Item 12 (reversed), “Grief [Eng ver.],” had negative item-rest correlations (-0.316 and -0.145). Cronbach’s α values if an item was deleted showed that removing Item 8 would increase α substantially from 0.236 to 0.566, while removing Item 12 would also raise α to 0.439.
3.3. Construct Validity
The confirmatory factor analysis (CFA) for the MAKS-M yielded a significant chi-square result (χ2(53) = 217.611, p < .001), indicating some model misfit (Table 4). The fit indices showed suboptimal values, with CFI = 0.712, TLI = 0.641, and NFI = 0.659, all below the commonly accepted 0.90 threshold. RMSEA was 0.124 and SRMR was 0.109, both exceeding recommended cut-offs (< 0.08) (Appendix E).
| Fit Index | Value | Interpretation |
|---|---|---|
| CFI | 0.712 | Below the acceptable threshold (<0.90) |
| TLI | 0.641 | Below the acceptable threshold (<0.90) |
| RMSEA | 0.124 | Poor fit; exceeds recommended cut-off (<0.08) |
| SRMR | 0.109 | Poor fit; exceeds recommended cut-off (<0.08) |
Notes: - Fit indices indicate that the hypothesized two-factor structure of the MAKS is not supported in the Malaysian context.
- Complete CFA model parameters and factor loadings are provided in Appendix E.
From factor loading analysis of each items, revealed that most items had statistically significant loadings on their respective factors (p < .05), except for Item 6 (reversed) “Most people with mental health problems… [English ver.]” in the knowledge subscale, and Items 8 (reversed) “Stress [Eng ver.] and 12 (reversed) “Grief [Eng ver.]” in the attitude subscale, which had low or negative loadings and non-significant p-values. Item 3 “Medication can be an effective treatment… [Eng ver.]”, 4 “Psychotherapy (e.g., talking therapy or counselling) can be an effective treatment… [Eng ver.], 9 “Schizophrenia [Eng ver.], and 10 “Bipolar Disorder (manic-depression) [Eng ver.]” showed the strongest loadings (> 0.50).
3.4. Convergent Validity
Table 5 presents the convergent validity analysis of the subscales, with correlations with BPIM. The Spearman’s correlation analysis indicated a significant positive relationship between the MAKS knowledge and MAKS attitude subscales (ρ = 0.307, p < .001). MAKS knowledge also showed a significant positive correlation with BIPM interest (ρ = 0.230, p < .001), and MAKS attitude correlated positively with BIPM interest as well (ρ = 0.218, p = .002). However, neither MAKS knowledge nor MAKS attitude correlated significantly with BIPM insight (p > .05).
| Variable | - | MAKS Knowledge | MAKS Attitude | BIPM Insight | BIPM Interest | ||||
|---|---|---|---|---|---|---|---|---|---|
| 1. MAKS knowledge | Spearman's rho | - | |||||||
| p-value | - | ||||||||
| 2. MAKS attitude | Spearman's rho | 0.307 | *** | - | |||||
| p-value | < .001 | - | |||||||
| 3. BIPM insight | Spearman's rho | -0.073 | -0.064 | - | |||||
| p-value | 0.300 | 0.366 | - | ||||||
| 4. BIPM interest | Spearman's rho | 0.230 | *** | 0.218 | ** | 0.089 | - | ||
| p-value | < .001 | 0.002 | 0.208 | - | |||||
Note: * p < .05, ** p < .01, *** p < .001.
4. DISCUSSION
4.1. Internal Consistency and Scale Reliability
The present findings should be interpreted not as a failed validation attempt, but as a methodological case study illustrating the psychometric vulnerabilities of direct scale transfer in cross-cultural mental health literacy measurement.
The low internal consistency observed in both subscales of the MAKS-M suggests deeper structural and contextual issues that extend beyond measurement error. One likely cause is the presence of reversed items, which are known to compromise reliability in cross-cultural adaptations, especially in multilingual contexts like Malaysia [12, 29]. The reversed items were retained during initial validation to maintain conceptual equivalence with the original MAKS and to empirically test whether previously reported item instability also emerged in the Malaysian context. Still, these items can create unintended cognitive load, where respondents-particularly those with varying literacy levels or second-language fluency-may misinterpret item direction, leading to inconsistent or contradictory responses. This semantic complexity may obscure the intended construct and undermine the coherence of the scale [12]. Additionally, the weak reliability indices observed may reflect not only the cognitive burden of reversed items in translated scales but also distributional characteristics; several reversed items demonstrated marked negative skew and peaked distributions, limiting variance and attenuating item-total correlations.
Another contributing factor may be the conceptual ambiguity within the subscales themselves. The knowledge subscale, for instance, includes items tapping both factual understanding and social perceptions of mental health (e.g., recognizing schizophrenia vs. beliefs about treatment effectiveness), which may not form a unidimensional construct. Similarly, the attitude subscale includes items ranging from general acceptance of mental health conditions to more specific views about treatment and disclosure [4, 12].
These findings reinforce prior arguments that the MAKS may be better suited for item-level or domain-specific interpretation rather than aggregate scoring, particularly in non-Western contexts. A scale with unreliable subscales may produce misleading conclusions about the public’s mental health knowledge and attitudes, particularly when used to evaluate interventions or track population-level changes. In research contexts, this limits the scale’s utility in hypothesis testing and weakens its psychometric credibility. In policy or educational settings, it may lead to erroneous assumptions about the effectiveness of mental health literacy campaigns or the prevalence of stigma [30, 31].
4.2. Item-Level and Structural Validity
The item-level analysis of the MAKS-M revealed inconsistencies that raise concerns about the scale’s structural validity. While some items showed acceptable alignment with their intended subscales, others-particularly the reversed items-performed poorly, with negative or near-zero item-rest correlations and non-significant factor loadings. These discrepancies suggest that certain items did not meaningfully contribute to the latent constructs they were intended to measure, pointing to potential issues in semantic clarity, conceptual alignment, or cultural relevance of specific statements [32].
One possible cause of weak item performance is the mismatch between item content and local interpretations of mental health. Items originally developed in Western contexts may not transfer seamlessly into the Malaysian cultural and linguistic environment, where beliefs, idioms, and stigma surrounding mental illness differ [33]. For example, terms like “treatment” or “disclosure” may carry different social connotations in collectivist cultures, where family reputation and social harmony play a stronger role in shaping attitudes. If the item content fails to reflect culturally embedded constructs of mental health knowledge and stigma, it may lack salience or be interpreted inconsistently by respondents [34].
Another contributing factor is item redundancy or ambiguity. Items that are too broadly worded may allow for varied interpretations, especially among respondents with differing educational backgrounds or mental health familiarity. Conversely, some items may be overly narrow or context-specific, limiting their generalizability and weakening their structural contribution. Moreover, the tendency of some items to elicit ceiling effects-where a large proportion of respondents choose the most favorable response-can reduce variance and inflate apparent item irrelevance, even if the content is meaningful [35].
Exploratory factor analysis (EFA) may be warranted to empirically reassess item groupings and potentially redefine subscale boundaries that better reflect local mental health literacy constructs. EFA was not initially prioritized because the primary objective was to test whether the original theoretical structure could be replicated in a new cultural context; only after structural non-equivalence was demonstrated does exploratory redevelopment become methodologically appropriate.
4.3. Model Fit and Factor Structure Comparison
The confirmatory factor analysis (CFA) of the MAKS-M revealed substantial misfit to the hypothesized two-factor structure, raising important concerns about the applicability of the original MAKS model in the Malaysian context [36]. In this context, CFA results are best understood as diagnostic evidence of structural misfit, highlighting the limits of direct construct transfer rather than as confirmatory tests of factorial validity.
While a two-factor structure-separating knowledge and attitude components-has been supported in some previous validations, these findings suggest that the theoretical distinction may not hold consistently across cultural settings [37]. Rather than viewing the poor model fit solely as model failure, these CFA results indicate that the original MAKS two-factor structure does not transfer adequately to the Malaysian context, suggesting a lack of structural equivalence.
Several factors may underlie the poor model fit. The inclusion of reversed items with weak or negative factor loadings (e.g., Items 6, 8, and 12) likely distorted the factorial structure [38]. The predominance of negatively skewed distributions, particularly for reversed and high-endorsement items, likely reduced item variability and impaired inter-item associations. These challenges align with prior reports that reversed items and ceiling effects commonly distort psychometric performance in cross-cultural mental health literacy instruments [38].
The relative homogeneity of the sample represents a design-linked psychometric constraint rather than merely a demographic limitation. The predominance of young, university-educated participants, combined with high prior exposure to mental health issues (81%), likely produced elevated endorsement of knowledge and attitude items. This resulted in pronounced ceiling effects and negative skewness, reducing item variance. Restricted variance attenuates inter-item correlations and covariance estimates, which in turn mechanically depress reliability coefficients and impair confirmatory factor analysis (CFA) model recovery. Thus, part of the observed psychometric instability may reflect limited score dispersion within this specific sample rather than purely structural flaws in the instrument.
The poor separation of subscales suggests that the MAKS-M may assess a hybrid construct that incorporates informational knowledge, personal beliefs, and perceived social norms. This raises the possibility that respondents are not reporting ‘knowledge’ in a positivist sense but rather articulating culturally mediated beliefs about mental health. Cultural norms and lived experiences may shape mental health beliefs in ways that blur the line between factual understanding and value-laden opinions [34]. For instance, endorsing a belief in the effectiveness of treatment may reflect both knowledge and optimism about recovery, which could reduce the clarity of the two-factor model.
Comparatively, previous adaptations of the MAKS in Asian populations have encountered similar difficulties. Studies in Singapore and China reported challenges in maintaining the original factor structure, often necessitating model respecification or item removal to achieve acceptable fit [14, 15]. These patterns suggest that the MAKS may require regional adaptation rather than direct translation, as its structural validity does not appear universally stable across contexts.
4.4. Cross Language Correlation
In this study, while full-scale back-translation procedures were followed, the results suggest that semantic and pragmatic differences between English and Malay may have compromised the integrity of certain items, particularly those with complex or nuanced phrasing.
The difficulties associated with reversed items in the MAKS-M likely reflect method effects rather than simple translation errors. Cross-cultural psychometric research has consistently demonstrated that negatively worded items may introduce systematic variance unrelated to the intended construct, often forming artificial method factors. In multilingual contexts, these effects are amplified by cognitive and linguistic asymmetry, as negation structures may alter sentence emphasis and processing demands [12, 28]. In Malay, explicit negative markers can increase syntactic complexity and pragmatic ambiguity, potentially triggering acquiescence or harmony-driven response tendencies [28]. Thus, the instability observed is not a critique of reversed wording per se, but evidence of interaction between language structure, cognitive load, and culturally patterned response styles [39].
Another challenge in cross-language correlation lies in the cultural framing of mental health concepts. For instance, terms such as “mental illness,” “treatment,” or “disclosure” may evoke different connotations across languages and cultures [40]. Even if direct translation is linguistically accurate, the psychological and social meanings embedded in these words may vary, affecting how respondents relate to and interpret each item [41].
The implications for cross-cultural research are significant. If conceptual equivalence is not adequately preserved, any observed differences in scores between linguistic groups may reflect measurement artifacts rather than true differences in mental health literacy. This limits the utility of the MAKS-M in multicultural studies or in evaluating interventions across linguistically diverse populations [41].
4.5. Implications for Cross-Cultural Application of MAKS
The findings of this study underscore the challenges of applying mental health literacy instruments across cultural contexts without rigorous adaptation. Although the MAKS was originally developed to assess universal aspects of mental health knowledge and stigma, its application in Malaysia revealed limitations that extend beyond linguistic translation.
In collectivist Malaysian settings, mental health understanding is influenced by family interdependence, moral attributions, and religious frameworks [34]. These factors reduce the distinction between what people believe to be true, what they feel socially expected to endorse, and what they personally understand. These cultural underpinnings influence not only the interpretation of mental health concepts but also the acceptability of certain attitudes and behaviours [42]. For example, questions about disclosure or treatment-seeking may invoke concerns about shame or social harmony, which are not explicitly addressed in the original MAKS. As such, items developed in Western settings may not resonate with or fully capture the lived experiences and stigma mechanisms present in non-Western societies [43].
4.6. Implications for Redevelopment
Rather than viewing these results solely as translation shortcomings, the findings highlight foundational measurement weaknesses within the MAKS framework. The inability of the MAKS-M to demonstrate acceptable psychometric performance underlines the need to reconceptualise mental health knowledge assessment in Malaysia from the ground up. The evidence indicates that future work should prioritise the redevelopment of item content rather than incremental revision. Psychometric instability in multiple international adaptations suggests that the MAKS construct architecture itself may lack robustness across cultural settings.
4.7. Contribution Beyond MAKS-M
Beyond evaluating the Malay version of the MAKS, this study offers broader methodological insights into cross-cultural mental health measurement. It demonstrates that reversed items are particularly vulnerable to linguistic and cultural distortion, often producing systematic psychometric failure rather than random noise. The findings highlight that mental health “knowledge” and “attitude” may not function as clearly separable constructs in non-Western contexts, where factual understanding, moral beliefs, and social norms are closely intertwined. By treating poor psychometric performance as informative rather than dismissible, this study illustrates the value of explicitly testing construct viability rather than assuming structural stability during scale adaptation.
5. STRENGTHS AND LIMITATIONS
One key strength lies in its comprehensive psychometric evaluation, employing a range of reliability indices (Cronbach’s α, McDonald’s ω, GLB), item-level diagnostics, and confirmatory factor analysis. This multi-method approach provided nuanced insights into the scale’s internal structure and performance. Additionally, the inclusion of convergent validity testing with the Balanced Index of Psychological Mindedness (BIPM) adds credibility to the interpretation of subscale associations, particularly with regard to the “interest” dimension of psychological mindedness.
The study also benefits from a relatively diverse participant pool in terms of educational and occupational background, although it was predominantly composed of young and university-educated individuals. The methodological rigor in translation-following standard forward- and back-translation procedures-adds value by ensuring at least a foundational level of linguistic equivalence between the original and Malay versions.
However, several limitations must be acknowledged. First and foremost, the bilingual administration of instruments, while intended to support cross-language comparison, may have introduced priming effects that influenced item interpretation and response consistency.
The second limitation relates to the distributional characteristics of several MAKS-M items. Item-level analyses revealed pronounced negative skewness and ceiling effects, particularly for items assessing recognition of common mental health conditions (e.g., depression, schizophrenia, bipolar disorder). Such skewed distributions reduce item variance and can attenuate inter-item correlations, thereby adversely affecting confirmatory factor analysis (CFA) results. As CFA using maximum likelihood estimation assumes approximate multivariate normality, deviations from normality may have contributed to the observed model misfit. These issues limit the current version’s suitability for research, policy evaluation, or community use without substantial revision or redevelopment.
Thirdly, the sample, while adequate in size, was not demographically representative of the broader Malaysian population. The high proportion of participants with prior exposure to mental health issues (over 80%) and tertiary education may have introduced a bias toward more favorable attitudes and higher knowledge levels, thus contributing to ceiling effects and limiting generalizability.
Fourth, the reliance on self-report measures introduces the possibility of social desirability bias, particularly in items related to mental health stigma. Respondents may have selected more socially acceptable answers, especially in a survey format without interviewer clarification. This may have obscured true variability in attitudes and knowledge, further complicating reliability and validity interpretation.
Finally, while this study focused on psychometric properties, it did not incorporate qualitative feedback on item comprehension or cultural relevance. Such insights could have enriched the interpretation of problematic items and informed more targeted revisions.
CONCLUSION
This study demonstrated why the MAKS, in its current form, does not transfer psychometrically across cultures, thereby highlighting the need for redevelopment rather than incremental translation. These findings provide empirical guidance for researchers engaged in cross-cultural measurement, particularly regarding the risks posed by reversed items and poorly delineated constructs. The MAKS-M, in its current iteration, falls short of acceptable psychometric standards and should not be used for composite scoring in Malaysia in its current form.
RECOMMENDATIONS
Based on the findings of this study, it is recommended that the Malay version of the Mental Health Knowledge Schedule (MAKS-M) undergo redevelopment before being adopted for widespread use in Malaysian research or practice. The current psychometric limitations-particularly poor internal consistency, misfitting factor structure, and problematic reversed items-underscore the need for both linguistic and conceptual revisions to improve the tool’s validity and reliability.
One of the most urgent adjustments involves the removal or rewording of reversed items (Items 6, 8, and 12). These items consistently produced negative item-rest correlations and weak factor loadings, suggesting that their negative phrasing may have introduced confusion or cognitive strain for respondents [44]. Future Malay adaptations of mental health literacy tools should avoid negatively worded items and consider rephrasing these items into positively worded statements while maintaining their intended construct. For example, instead of negatively phrased items that require mental reversal (e.g., “Most people with mental health problems go to prison”), a direct but positively framed alternative (e.g., “People with mental health problems are not more likely to go to prison”) may improve interpretability without sacrificing meaning.
Additionally, several items may require conceptual clarification or cultural adaptation to better align with local beliefs and practices around mental health. Items that reference treatment, disclosure, or stigma should be evaluated for cultural salience, perhaps by incorporating commonly understood terms or examples that reflect Malaysian mental health realities [45]. This could include references to family involvement in care decisions, religious interpretations of illness, or community-level stigma, which may not be captured in the original item phrasing.
Future validation designs should draw from more demographically diverse groups-including rural, older, and less-educated populations-to ensure adequate variability and to reduce ceiling effects. Additionally, qualitative methods such as cognitive interviews, focus groups, and expert panel reviews should be integrated into future validation phases. These approaches can help identify misunderstood items, ambiguous language, or culturally incongruent content. Exploratory factor analysis (EFA) is also recommended in the early stages of revision to empirically explore the underlying structure of the scale and to assess whether the original two-factor model remains appropriate, or whether an alternative configuration better reflects local constructs of mental health literacy.
Future research should treat the MAKS as a conceptual starting reference rather than a scale ready for adaptation. Item-level redevelopment informed by qualitative and cross-cultural methods may be required to produce a psychometrically stable measure of mental health knowledge. Any endeavor of MAKS validation should include more demographically diverse samples to enhance the generalizability of the findings. Validation in populations varying by age, education level, geographic location (including rural areas), and cultural background within Malaysia will be essential to ensure the scale functions reliably across subgroups.
AUTHORS’ CONTRIBUTIONS
It is hereby acknowledged that all authors have accepted responsibility for the manuscript's content and consented to its submission. They have meticulously reviewed all results and unanimously approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| CFA | = Confirmatory Factor Analysis |
| MAKS-M | = Mental Health Knowledge Schedule |
| BIPM | = Balanced Index of Psychological |
| GLB | = Mindedness Greatest Lower Bound |
| RMSEA | = Root Mean Square Error of Approximation |
| SRMR | = Standardized Root Mean Square Residual |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval for this study was obtained from the Research Ethics Committee, University Malaysia Sabah, Malaysia, with approval code JKEtika 4/25(27).
HUMAN AND ANIMAL RIGHTS
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written informed consent was obtained from all participants for their participation in the study, and all data were anonymized prior to analysis and reporting. Therefore, no additional consent for publication of individual data is required.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of this article are available in the Zenodo repository at https://doi.org/10.5281/zenodo.21126479.
ACKNOWLEDGEMENTS
Declared none.
APPENDIX
| Item | English MAKS | Malay Translation |
|---|---|---|
| Mental Health Knowledge Schedule | Jadual Pengetahuan Mengenai Kesihatan Mental | |
| 1 | Most people with mental health problems want to have paid employment. | Ramai orang yang ada gejala kesihatan mental ingin pekerjaan yang dibayar gaji. |
| 2 | If a friend had a mental health problem, I know what advice to give them to get professional help | Kalau kawan saya ada gejala kesihatan mental, saya tahu nasihat yang boleh diberikan untuk mereka mendapatkan bantuan pakar. |
| 3 | Medication can be an effective treatment for people with mental health problems | Mengambil ubat dari hospital berkesan untuk merawat gejala kesihatan mental. |
| 4 | Psychotherapy (eg talking therapy or counseling) can be an effective treatment for people with mental health problems | Psikoterapi (kaunseling dan terapi meluahkan perasaan) berkesan untuk merawat gejala kesihatan mental. |
| 5 | People with severe mental health problems can fully recover | Mereka yang mempunyai gejala kesihatan mental yang teruk boleh sembuh sepenuhnya. |
| 6 | Most people with mental health problems go to a healthcare professional to get help | Ramai orang yang ada gejala kesihatan mental dapatkan bantuan dari pakar perubatan. (reversed) |
| 7 | Depression | Kemurungan |
| 8 | Stress | Stres (reversed) |
| 9 | Schizophrenia | Skizofrenia |
| 10 | Bipolar Disorder (manic-depression) | Kecelaruan Bipolar (episod mania - kemurungan) |
| 11 | Drug addiction | Ketagihan Dadah |
| 12 | Grief | Kehibaan (Perasaan kehilangan sesuatu yang dikasihi) (reversed) |
| Arahan: Bagi pernyataan 1 - 6, sila tandakan pada satu petak sahaja. Gejala kesihatan mental merujuk kepada keadaan-keadaan yang sepatutnya dirawat oleh ahli-ahli penjagaan kesihatan. | |||||||
|---|---|---|---|---|---|---|---|
| Sangat setuju | Agak setuju | Neutral | Kurang setuju | Sangat Tidak Setuju | Tidak Tahu | ||
| 1 | Ramai orang yang ada gejala kesihatan mental ingin pekerjaan yang dibayar gaji. | ||||||
| 2 | Kalau kawan saya ada gejala kesihatan mental, saya tahu nasihat yang boleh diberikan untuk mereka mendapatkan bantuan pakar. | ||||||
| 3 | Mengambil ubat dari hospital berkesan untuk merawat gejala kesihatan mental. | ||||||
| 4 | Psikoterapi (kaunseling dan terapi meluahkan perasaan) berkesan untuk merawat gejala kesihatan mental. | ||||||
| 5 | Mereka yang mempunyai gejala kesihatan mental yang teruk boleh sembuh sepenuhnya. | ||||||
| 6 | Ramai orang yang ada gejala kesihatan mental dapatkan bantuan dari pakar perubatan. | ||||||
| Arahan: Nyatakan sama ada kondisi berikut adalah jenis penyakit mental dengan menandakan satu kotak sahaja. | |||||||
| 7 | Kemurungan | ||||||
| 8 | Stres | ||||||
| 9 | Schizophrenia | ||||||
| 10 | Kecelaruan Bipolar (episod mania - kemurungan) | ||||||
| 11 | Ketagihan Dadah | ||||||
| 12 | Kehibaan (Perasaan kehilangan sesuatu yang dikasihi) | ||||||
| Item | Mean | Std. Deviation | Skewness | Std. Error of Skewness | Kurtosis | Std. Error of Kurtosis | Minimum | Maximum |
|---|---|---|---|---|---|---|---|---|
| 1. Ramai orang yang ada gejala kesihatan mental ingin pekerjaan yang dibayar gaji. | 3.985 | 0.876 | -0.730 | 0.171 | 0.638 | 0.340 | 1.000 | 5.000 |
| 2. Kalau kawan saya ada gejala kesihatan mental, saya tahu nasihat yang boleh diberikan untuk mereka mendapatkan bantuan pakar. | 3.833 | 0.809 | -0.534 | 0.171 | 0.303 | 0.340 | 1.000 | 5.000 |
| 3. Mengambil ubat dari hospital berkesan untuk merawat gejala kesihatan mental. | 3.897 | 0.887 | -0.656 | 0.171 | 0.460 | 0.340 | 1.000 | 5.000 |
| 4. Psikoterapi (kaunseling dan terapi meluahkan perasaan) berkesan untuk merawat gejala kesihatan mental. | 4.187 | 0.774 | -0.661 | 0.171 | -0.081 | 0.340 | 2.000 | 5.000 |
| 5. Mereka yang mempunyai gejala kesihatan mental yang teruk boleh sembuh sepenuhnya. | 3.310 | 0.958 | 0.024 | 0.171 | -0.464 | 0.340 | 1.000 | 5.000 |
| 6. Ramai orang yang ada gejala kesihatan mental dapatkan bantuan dari pakar perubatan. (reversed) | 2.837 | 1.103 | 0.081 | 0.171 | -0.900 | 0.340 | 1.000 | 5.000 |
| 7. Kemurungan | 4.527 | 0.692 | -1.504 | 0.171 | 2.174 | 0.340 | 2.000 | 5.000 |
| 8. Stres (reversed) | 2.764 | 1.260 | 0.095 | 0.171 | -1.110 | 0.340 | 1.000 | 5.000 |
| 9. Skizofrenia | 4.586 | 0.755 | -1.863 | 0.171 | 3.158 | 0.340 | 1.000 | 5.000 |
| 10. Kecelaruan Bipolar (episod mania - kemurungan) | 4.650 | 0.638 | -1.852 | 0.171 | 3.033 | 0.340 | 2.000 | 5.000 |
| 11. Ketagihan Dadah | 3.616 | 1.255 | -0.440 | 0.171 | -1.023 | 0.340 | 1.000 | 5.000 |
| 12. Kehibaan (Perasaan kehilangan sesuatu yang dikasihi) (reversed) | 3.463 | 1.263 | -0.362 | 0.171 | -0.987 | 0.340 | 1.000 | 5.000 |
Scale Reliability Statistics: Knowledge subscale.
| Estimate | McDonald's ω | Cronbach's α | Greatest Lower Bound |
|---|---|---|---|
| Point estimate | 0.396 | 0.262 | 0.480 |
| 95% CI lower bound | 0.284 | 0.089 | 0.408 |
| 95% CI upper bound | 0.509 | 0.409 | 0.606 |
Note: The following item correlated negatively with the scale: Item6_reversed.
| Estimate | McDonald's ω | Cronbach's α | Greatest Lower Bound |
|---|---|---|---|
| Point estimate | 0.444 | 0.236 | 0.646 |
| 95% CI lower bound | 0.347 | 0.051 | 0.534 |
| 95% CI upper bound | 0.541 | 0.391 | 0.742 |
Note: The following item correlated negatively with the scale: Item8_reversed.
| If item dropped | ||
|---|---|---|
| Item | Cronbach's α | Item-rest correlation |
| Item1 | 0.175 | 0.183 |
| Item2 | 0.210 | 0.141 |
| Item3 | 0.080 | 0.295 |
| Item4 | 0.013 | 0.413 |
| Item5 | 0.284 | 0.046 |
| Item6_reversed | 0.500 | -0.200 |
| If item dropped | ||
|---|---|---|
| Item | Cronbach's α | Item-rest correlation |
| Item7 | 0.026 | 0.419 |
| Item8_reversed | 0.566 | -0.316 |
| Item9 | -0.072 | 0.524 |
| Item10 | -0.036 | 0.555 |
| Item11 | 0.027 | 0.259 |
| Item12_reversed | 0.439 | -0.145 |
Appendix E: Full CFA factor loading table with fit indices
| Model | Χ2 | df | p |
|---|---|---|---|
| Baseline model | 637.323 | 66 | |
| Factor model | 217.611 | 53 | < .001 |
Note: The estimator is ML.
| Index | Value |
|---|---|
| Comparative Fit Index (CFI) | 0.712 |
| Tucker-Lewis Index (TLI) | 0.641 |
| Bentler-Bonett Normed Fit Index (NFI) | 0.659 |
| Root mean square error of approximation (RMSEA) | 0.124 |
| Standardized root mean square residual (SRMR) | 0.109 |
| Goodness of fit index (GFI) | 0.991 |
| 95% Confidence Interval | |||||||
|---|---|---|---|---|---|---|---|
| Factor | Indicator | Estimate | Std. Error | z-value | p | Lower | Upper |
| Knowledge | Item1 | 0.296 | 0.076 | 3.888 | < .001 | 0.147 | 0.446 |
| Item2 | 0.265 | 0.071 | 3.718 | < .001 | 0.125 | 0.404 | |
| Item3 | 0.531 | 0.085 | 6.273 | < .001 | 0.365 | 0.696 | |
| Item4 | 0.504 | 0.076 | 6.648 | < .001 | 0.355 | 0.652 | |
| Item5 | 0.209 | 0.092 | 2.277 | 0.023 | 0.029 | 0.388 | |
| Item6_reversed | -0.119 | 0.099 | -1.202 | 0.229 | -0.312 | 0.075 | |
| Attitude | Item7 | 0.409 | 0.046 | 8.908 | < .001 | 0.319 | 0.498 |
| Item8_reversed | 0.130 | 0.093 | 1.400 | 0.162 | -0.052 | 0.311 | |
| Item9 | 0.690 | 0.044 | 15.692 | < .001 | 0.604 | 0.776 | |
| Item10 | 0.575 | 0.037 | 15.399 | < .001 | 0.501 | 0.648 | |
| Item11 | 0.306 | 0.091 | 3.358 | < .001 | 0.127 | 0.484 | |
| Item12_reversed | -0.080 | 0.093 | -0.865 | 0.387 | -0.262 | 0.102 | |

