All published articles of this journal are available on ScienceDirect.

Humor Training Program on Sense of Humor among Older Adults: A Randomized Controlled Trial
Abstract
Introduction:
Several studies have a well-documented positive association between sense of humor and physical and mental well-being in later life. However, there is evidence to indicate that sense of humor declines with age. This study was conducted to examine humor training program on the sense of humor among older adults.
Methods:
This community-based randomized controlled trial study was conducted in 2019. There were 18 older adults in the intervention group and 20 older adults in the control group. The intervention group received the 7 Humor Habits Program in eight training sessions, whereas the control group was waitlisted. The Multidimensional Sense of Humor Scale (MSHS) was used to measure the sense of humor before and after the intervention. A series of paired samples t-tests and difference-in-differences approach using IBM SPSS Version 23.0 were conducted to assess changes from pre-test to post-test. The significance level of p ≤ .05 was considered for the statistical analysis.
Results and Discussion:
The mean age of the participants in the intervention and control groups was 66.50, (SD=6.14) and 67.60, (SD= 5.64) years, respectively. The results of a series of paired samples t-tests revealed a statistically significant increase in the total score of sense of humor from pre-test (M =77.28, SD = 13.62) to post-test (M=101.11, SD=17.06), (t= -6.77, p<.001), in intervention group. Other paired samples t-tests showed statistically significant changes from pre-test to post-test for subscales of humor including enjoyment of humor (t= -4.59, p<.001), laughter (t= -7.83, p<.001), verbal humor (t= -4.73, p<.001), finding humor in everyday life (t= -4.19, p<.001), laughing at yourself (t= -6.36, p<.01), and humor under stress (t= -2.54, P≤.05) in intervention group. Moreover, the results of the difference-in-differences approach revealed a significant increase in the sense of humor for the intervention group compared to the control group (F=43.54, p<.001). No statistically significant changes were observed in any outcome variables in the control group.
Conclusion:
The results of this study provided support that the sense of humor can be improved using a training program in later life.
1. INTRODUCTION
According to the United Nations, there are currently around 962 million people aged 60 years and above in the world, comprising 13% of the global population. It is projected that the number of older people in the world will reach 1.4 billion by 2030, 2.1 billion by 2050, and rise to 3.1 billion by 2100, with a growing rate of about 3% per year [1]. Iran, with 9.3 percent older adults aged 60 years and over in 2016, like many other countries around the world, is heading towards declining fertility rates combined with improvements in life expectancy [2]. As the population ages, identifying novel ways to maintain and promote the well-being of older adults is imperative.
According to the gerontological and geriatric literature, one of the most important contributing factors to older adults’ well-being is a sense of humor. It has been defined in the literature as a cognitive ability to remember, create and understand jokes, an appreciation of humor, a tendency to laugh, a habitual cheerfulness, and a coping strategy [3].
The sense of humor has three meanings. A person is humorous if: 1- people laughed at what he/she does; 2- he/she laughs a lot and is easily amused; 3- he/she narrates funny stories and amuses others [4]. Moreover, humor refers to the willingness to experience or express what is amusing and funny [5].
There is a growing body of evidence which shows that humor improves physical and mental health, and enhances a positive worldview [6-9]. It has been considered as the most natural and cost-free method of reducing stress, anxiety, and tension. It creates psychological, emotional, and physiological changes that result in people having control over their lives [10]. The results of a study conducted by Morse et al. [11] to examine the effect of improvisation comedy on healthy older adults emerged the common themes including increased positivity, increased sense of comfort and ease with the unexpected, a sense of self-development and self-awareness, and a feeling of acceptance by their social group. The authors stated that humor combats several common geriatric conditions, such as depression, stress, and isolation. The other studies have documented that sense of humor is a health-protecting cognitive coping resource [9] that increases the probability of survival into retirement [12] and assists in the process of aging, particularly in improving health, reducing stress, and improving psychological well-being and life satisfaction among older adults [10]. The studies have examined the effect of humor on older adults, which found that humor may play a role in alleviating death anxiety [13], providing a sense of hopefulness [14], reducing pain and providing a sense of camaraderie [15], and improving older adults’ attitude about the aging process [10]. Thus, it can be found from the literature that sense of humor not only induces positive emotions, but also it may help to reduce negative emotions and stress [8].
Although the positive effect of humor on older adults has been documented by several studies, unfortunately, it should be noted that there is evidence to indicate that ability to produce, appreciate, and comprehend humor declines with age [12, 16-18]. The most important issue of humor research is that many of these studies have conducted in the cross-sectional design and conducted experimental studies did not focus on older adults.
Generally, although humor is a universal phenomenon, the way people use and express humor is strongly influenced by cultural norms, beliefs, attitudes, and values [4, 19, 20]. Thus, humor training can be influenced by culture. With regard to the positive effect of sense of humor in later life and its culture-based nature, it is imperative to find ways to maintain and improve a sense of humor. This study, therefore, has been conducted to examine humor training programs on the sense of humor among older adults.
2. METHODS
2.1. Study Design
The present community-based Randomized Controlled Trial (RCT) with a two-group design was conducted in 2019. The CONSORT statement was employed in designing the study and reporting results [21]. Written informed consent was obtained from all participants after providing information about the purpose of the study.
2.2. Participants
The participants were selected from health centers using electronic medical records in Jam city. The city of Jam is located on the southeast of the Bushehr province, Iran. It is noteworthy to mention that mostly all elderly people have a medical record. According to the national census in 2016, its population is 70,051.
2.3. Sample Characteristics
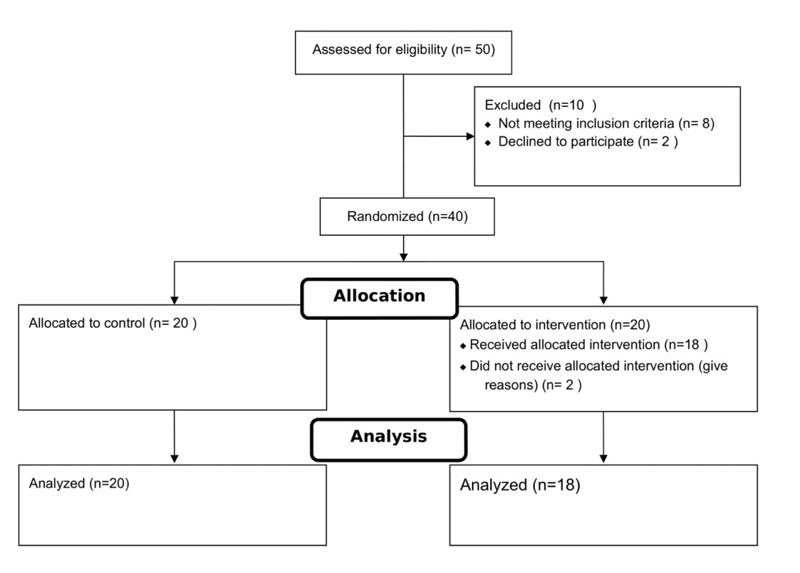
A total of 50 health records of elderly people aged 60 years and over were randomly selected from Jam health centers. Forty-six elderly people were contacted by telephone for participation. Forty-two persons were eligible to participate in the study. The inclusion criteria were aged 60 years and over, with no major visual and hearing impairments, and lack of cognitive disorders. The exclusion criteria were refusing to participate, experiencing any psychosocial problems during the study, and not attending two sessions. The study flow diagram is presented in Fig. (1). In the end, 40 older adults met the inclusion criteria for participating in the study, of which, 20 persons were randomly assigned to the intervention and 20 persons to the control group and assessed at baseline. The study sample was assigned to either the intervention group or the control group using a simple random sampling technique. The randomization was performed using an online random number generator website (http://www.randomizer.org/ form.htm). Two elderly people of the intervention group left the study (10%), which are less than 20 percent, so no replacement of missing cases was needed.
2.4. Measurement
The sense of humor was measured using the Multidimensional Sense of Humor Scale (MSHS) before and after the eight-week intervention. The MSHS is a 24-item scale with a 5-point Likert format from 0 = strongly disagree coded zero to strongly agree coded 4. The possible range is from 0 to 96 and a higher overall score indicates a higher sense of humor [22]. The internal consistency reliability of the MSHS as a whole and its domains was calculated in this study. The Cronbach’s Alpha reliability coefficient for the MSHS was found to be 0.94. The Cronbach’s Alpha values for the MSHS subscales, including enjoyment of humor, laughter, verbal humor, finding humor in everyday life, laughing at yourself, and humor under stress, were obtained as 0.68, 0.74, 0.76, 0.78, 0.81, and 0.94, respectively, demonstrating good internal consistency.
| Session | Aim | Content |
| 1 | Identify the nature of your sense of humor. |
Culture and sense of humor. Description of the participants' humor preferences. |
| 2 | Become less serious and more playful about life. | The adverse effects of seriousness on everyday life. The impact of playfulness on coping with stress. |
| 3 | Laughter heartily and recitation jokes. | Positive effects of laughter. |
| 4 | Improve your ability to tell jokes. | Practicing the creation of jokes. |
| 5 | Find the funny side of things happening in everyday life. |
Consciously searching for humor in daily situations. |
| 6 | Learn to laugh at yourself. | How to start laughing at yourself humorous perspective on personal weaknesses. |
| 7 | Change of perspective on difficult situations. | Effects of humor on stress. How to practice finding humor in stressful situations. |
| 8 | Use steps 1–7 to cope with stress. | Use steps 1–7 to cope with stress. |
2.5. Intervention
The 7-Humor Habits Program (7HHP) was used in this study. The 7HHP (Initially called the 8 Step Humor Training Program) is a standardized training program, which can be implemented individually using a manual or in a group setting guided by a moderator [8]. It was developed by McGhee for strengthening key humor habits and skills. The 7HHP consists of seven core habits including surround yourself with humor, cultivate a playful attitude, laugh more often, create your own verbal humor, look for humor in daily life, laugh at yourself, find humor in the midst of stress [23].
2.6. Training and Procedure
Participants were recruited via health records. After showing interest in the study, they were informed about the study procedure and informed consent was obtained. Then, participants were asked to complete the baseline measures.
The intervention group received the 7HHP in eight training sessions of two hours length, coupled with home assignments. The group sessions included 1) Characterize your own sense of humor, 2) Become less serious and more playful about life, 3) Work on your belly laugh, 4) Improve your ability to tell jokes, 5) Create your own spontaneous humor, 6) Find humor in daily life, 7) Learn to laugh at yourself, 8) Use all of the above to cope with stress. The sessions were facilitated by a qualified psychologist. Table 1 summarizes the content of the sessions.
With respect to the evidence, it indicates that humor is a universal phenomenon, however, individuals from different cultures may see humor in different ways [19]; in the first session, participants were taught about the importance of humor based on their culture. 2.7 Ethical considerations
The current study was conducted according to the Declaration of Helsinki, World Medical Association (WMA) and approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran (IR.USWR.REC.1398.153). Written informed consent was obtained from all participants.
2.7. Statistical Analysis
The IBM SPSS Version 23.0 was used and the significance level of p ≤ 0.05 was considered for the statistical analysis. Descriptive analysis was performed with measures of central tendencies and dispersion. A Shapiro–Wilk test was performed to confirm proximity with a normal distribution. A series of independent-samples t-test and chi-square tests were used in the baseline analysis. A series of paired samples t-test and difference-in-differences approach were conducted to assess changes from pre-test to post-test. For the analyses, only participants that completed at least six of the eight training meetings were included.
3. RESULTS
A total of 38 community-dwelling older adults with a mean age of 67.05 years (SD=5.83) (ranging from 60 to 80 years) were included in the study as intervention and control groups.
The mean age of the participants was found to be 65.15 (SD=4.25). Intervention group consisted of 18 community-dwelling older adults (age: M = 66.50, SD = 6.14; 7 males, 11 females) and the waiting control group consisted of 20 community-dwelling older adults (age: M = 67.60, SD=5.64; 8 males, 12 females). The results of the independent t-test showed no significant difference between groups in the means of age (t(36)=-0.58, p=.568).
The sociodemographic and health characteristics of the sample by groups are presented in Table 2 The results of the bivariate analysis revealed no statistically significant difference between the intervention group and the control group in terms of age, sex, level of education, marital status, living arrangement, and chronic medical conditions (Table 2).
A series of independent-samples t-test were conducted to assess two groups at baseline regarding the sense of humor score. Table 3 shows the baseline scores on the sense of humor of the study participants. As shown in Table 3, no statistically significant difference was observed between the intervention group and the control group at baseline except for “laughing at yourself” which was higher in the control group (P ≤ 0.05).
| Variable | Category | Intervention | Control | χ2 | p | ||
| n | % | n | % | ||||
| Sex | Male | 7 | 46.7 | 8 | 53.3 | 0.01 | 0.944 |
| Female | 11 | 47.8 | 12 | 52.2 | |||
| Education | No Formal Education | 8 | 42.1 | 11 | 57.9 | 0.42 | 0.516 |
| Formal Education | 10 | 52.6 | 9 | 47.4 | |||
| Marital Status | Married | 12 | 46.2 | 14 | 53.8 | 0.05 | 0.825 |
| Unmarried | 6 | 50 | 6 | 50 | |||
| Living Arrangement | Alone | 2 | 50 | 2 | 50 | 0.05 | 0.976 |
| Spouse | 12 | 46.2 | 14 | 53.8 | |||
| Children | 4 | 50 | 4 | 50 | |||
| Chronic Medical Conditions | Yes | 10 | 38.5 | 16 | 61.5 | 2.6 | .106 |
| No | 8 | 66.7 | 4 | 33.3 | |||
| Variable | Intervention | Control | t | P | ||
| Mean | SD | Mean | SD | |||
| Enjoyment of Humor | 11.17 | 3.6 | 11.15 | 2.85 | 0.02 | 0.987 |
| Laughter | 10.17 | 2.75 | 12.1 | 3.92 | -1.74 | 0.09 |
| Verbal Humor | 8.94 | 1.55 | 9.85 | 3.39 | -1.04 | 0.306 |
| Finding Humor in Everyday Life | 14.28 | 3.34 | 15.5 | 3.52 | -1.1 | 0.281 |
| Laughing at Yourself | 13.11 | 2.85 | 15.65 | 4.48 | -2.06 | 0.047 |
| Humor Under Stress | 14.61 | 4.57 | 13.55 | 5.26 | 0.66 | 0.513 |
| Total Humor | 72.28 | 13.62 | 77.8 | 17.63 | -1.07 | 0.291 |
| Group | Variable | Pre Test | Post Test | t | P | ||
| Mean | SD | Mean | SD | ||||
| Intervention | Enjoyment of Humor | 11.17 | 3.6 | 15.22 | 4.11 | -4.59 | P<0.001 |
| Laughter | 10.17 | 2.75 | 18.11 | 3.1 | -7.83 | P<0.001 | |
| Verbal Humor | 8.94 | 1.55 | 12.72 | 3.1 | -4.73 | P<0.001 | |
| Finding Humor in Everyday Life | 14.28 | 3.34 | 17.5 | 3.26 | -4.19 | P<0.01 | |
| Laughing at Yourself | 13.11 | 2.85 | 19.33 | 3.43 | -6.36 | P<0.001 | |
| Humor Under Stress | 14.61 | 4.57 | 18.22 | 4.49 | -2.54 | P≤0.05 | |
| Total Humor | 72.28 | 13.62 | 101.11 | 17.06 | -6.77 | P<0.001 | |
| Control | Enjoyment of Humor | 11.15 | 2.85 | 11.05 | 3 | 0.35 | 0.733 |
| Laughter | 12.1 | 3.92 | 12.45 | 3.39 | -1.68 | 0.11 | |
| Verbal Humor | 9.85 | 3.39 | 10 | 3.18 | -0.9 | 0.379 | |
| Finding Humor in Everyday Life | 15.5 | 3.52 | 14.65 | 3.84 | 1.56 | 0.135 | |
| Laughing at Yourself | 15.65 | 4.48 | 15.7 | 4.07 | -0.22 | 0.825 | |
| Humor Under Stress | 13.55 | 5.26 | 13.9 | 4.85 | -1.32 | 0.201 | |
| Total Humor | 77.8 | 17.63 | 77.75 | 16.82 | 0.06 | 0.951 | |
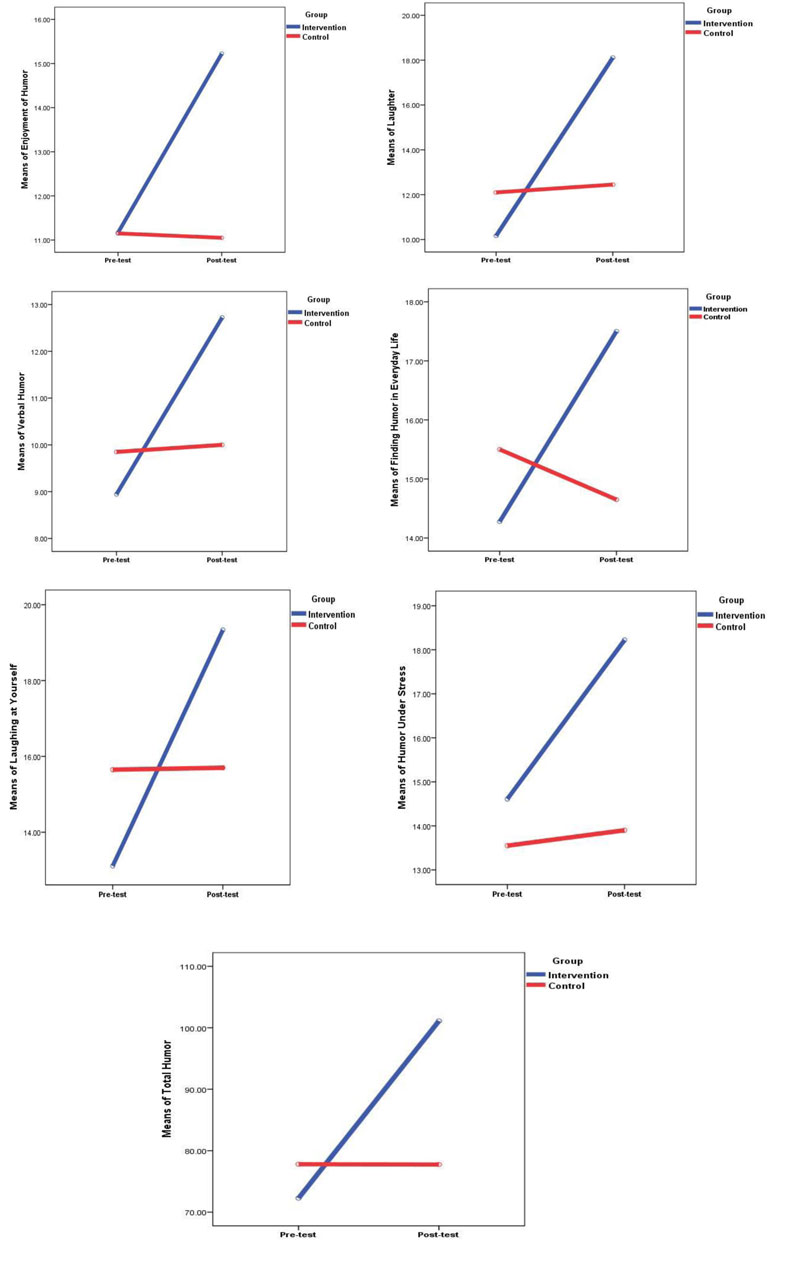
A series of paired samples t-test were conducted to evaluate the impact of the intervention on older adult’s scores on the sense of humor and its subscales. Table 4 shows the results of paired samples t-tests by study groups. As shown in Table 4, a statistically significant increase was observed in total score of sense of humor from Pre-test (M =77.28, SD = 13.62) to Post-test (M = 101.11, SD=17.06), t= -6.77, p<.001, in the intervention group. Results of other paired t-tests showed statistically significant changes from pre-test to post-test for enjoyment of humor (t= -4.59, p<.001), laughter (t= -7.83, p<.001), verbal humor (t= -4.73, p<.001), finding humor in everyday life (t= -4.19, p<.001), laughing at yourself (t= -6.36, p<.01), and humor under stress(t= -2.54, P≤.05) in intervention group. As shown in Table 4, no statistically significant changes were observed in any outcome variables from pre-test to post-test in the control group. Fig. (2) shows changes of the sense of humor and its subscales from pretest to post-test in both groups.
Additionally, a difference-in-differences analysis using an adjusted general linear model was carried out to compare two intervention and control groups in terms of a sense of humor before and after the intervention. The analysis revealed a significant increase in the sense of humor for the intervention group compared to the control group (F=43.54, p<.001), after controlling for age, sex, level of education, marital status, and chronic medical conditions. The mean score of sense of humor increased from 77.28 to 101.11 (30.8%) among the intervention group, while the average score of the sense of humor for the control group did not change substantially over time.
4. DISCUSSION
Humor has been conceptualized both as a cognitive ability (humor comprehension) and as an aesthetic response (humor appreciation) [24]. It has been considered a successful coping technique that can provide a more optimistic attitude towards life [25]. According to McGhee [26], humor can allow individuals to manage serious situations by redefining the circumstances as less threatening.
The current study investigated the effectiveness of the 7 humor habits on a sample of older adults in a randomized controlled trial. The intervention group received McGhee’s eight-week humor training. For the intervention group, the sense of humor increased from pre to post intervention. This indicated that the sense of humor could be malleable through a humor training program. The findings from the current study are consistent with some previous studies which found the 7HHP effectively foster humor [8, 25, 27].
In their study, Ruch, Hofmann [8] found that while the exposure to humor may increase the cheerfulness and decrease the seriousness, it cannot increase the sense of humor. In other words, unsystematic exposure to humor may result in a short-term induction of humor-related mood; it does not foster the sense of humor.
A growing body of research has documented the positive relationships between sense of humor and well-being. Individuals with a higher sense of humor are more likely to be able to reframe adverse events [25].
As people age, their cognitive abilities, such as conceptual reasoning, memory, and processing speed, gradually decline. It has been found that fluid intelligence, which refers to abilities involving executive function, processing speed, memory, and psychomotor, peaks in the third decade of life and then declines [28]. Humor requires many different cognitive functions particularly fluid cognitive abilities, which decline with age [29]. With regards to the bulk of evidence that indicates training improves cognitive function [30-32], it can be postulated that the humor training program may enhance the cognitive vitality of elderly people, consequently results in improving a sense of humor.
CONCLUSION
While several studies have documented humor as a potent predictor of life satisfaction and well-being, there is evidence indicating a sense of humor declines with age [33]. In addition to the declining humor in old age, eastern culture is less likely to use self-enhancing humor and may deprecate humor [19]. Therefore, elderly people need to be trained to enhance their sense of humor. The results of this study underline the importance of training on a sense of humor among the elderly. Our findings support the previous studies conducted by Jiang, Li [19] and Ruch, Hofmann [8] who found humor can be trained in old age and improved by standardized programs. It is suggested that the applicability of the program needs to be tested further in future studies in different settings.
LIMITATIONS
Like other research, this study is not free of limitations which need to be acknowledged. Although this study attempted to use rigorous methodology, it is impossible to eliminate all threats to the study. The first limitation of this study was the relatively small sample size due to the limited number of participants per group in group therapy, which is limited to a maximum of 15 persons per group [34]. Secondly, the limitation that should be acknowledged is that only a self-report method was used to collect data, it is suggested that in the future studies, a peer-rating method will be used to complement the self-reported humor.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran under ethical approval no (IR.USWR.REC.1398.153).
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Written informed consent was obtained from all the participants when they were enrolled.
STANDARDS OF REPORTING
CONSORT guidelines have been followed.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
This study was supported by grant No 1961 at the University of Social Welfare & Rehabilitation Sciences, Tehran, Iran.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

