All published articles of this journal are available on ScienceDirect.

Mindfulness-Based Eudaimonic Enhancement for Well-Being of Individuals with Alcohol-Dependence: A Pilot Randomized Controlled Study
Authors Info & Affiliations
Abstract
Background:
Theoretically, mindfulness or the non-judgmental awareness of the present generates eudaimonic well-being. Mindfulness-based interventions are effective for addictions like alcohol-dependence but its well-being outcomes should be validated empirically.
Objectives:
Current pilot study intended to explore the feasibility of a novel intervention, Mindfulness-Based Eudaimonic Enhancement Training (MEET), among individuals undergoing treatment for alcohol-dependence at an Integrated Rehabilitation Centre for Addicts (IRCA), Kerala, India.
Methods:
The experimental group (N=12) was administered with the intervention and Treatment as Usual (TaU) while the control group (N=12) received TaU alone. Obtained data were analysed using independent sample t-test and paired sample t-test.
Results:
After intervention the experimental group had reported better mindfulness, eudaimonic well-being, hedonic well-being, and flourishing. The results delineate the efficacy of the intervention as a mindfulness-based positive psychology intervention that enhances well-being and flourishing.
Conclusion:
This is the first study reporting the efficacy of a mindfulness-based intervention aimed exclusively at eudaimonic enhancement that showed promising impact among individuals with alcohol-dependence. The study contributes to the existing scientific literature, on the role of well-being and its enhancement for the effective treatment of addiction and relapse prevention.
1. INTRODUCTION
There are two major perspectives on human well-being – hedonia and eudaimonia [1-3]. Believed to have originated in Greece, the Aristippian concept of hedonia refers to “the pursuit and/or experience of pleasure, enjoyment, comfort, and reduced pain”. On the contrary, the Aristotelian concept of eudaimonia is “the pursuit, manifestation, and/or experience of virtue, personal growth, self-actualization, flourishing, excellence, and meaning” [4]. Hedonia is the tendency to seek pleasure and comfort while avoiding or escaping pain. Compared to eudaimonia, hedonia is easier to define and measure [5, 6]. Medical and pharmacological therapies primarily focus on hedonic well-being or alleviation of pain and elevation of pleasure. Psychotherapies too focus on improving hedonic well-being, largely ignoring the human needs that greatly exceed mere hedonia. Meanwhile, positive psychology, “the scientific study of what makes life most worth living” [7], addresses how eudaimonia shall be enhanced [8, 9], however, there is an imperative need of an intervention that exclusively focuses on eudaimonic enhancement. No adverse consequences of eudaimonia are reported, but excessive hedonic indulgence is neither pleasant nor healthy in the long run. A consequence of such imbalanced hedonic tendency is addiction [10, 11].
One of the highly prevalent addictions that pose colossal damage to health and well-being of global community is alcohol use and related disorders [12]. The major reasons for alcohol consumption encompass avoidance of negative experiences and pleasure-seeking. It is evident in neuroimaging studies that alcohol stimulates activation in the rewarding system and reduces activation in fear-arousing limbic region, thereby decreasing anxiety [13, 14]. In short, people drink either to forget unpleasant experiences [15, 16] or to derive pleasure [17]. Whatsoever, alcohol-dependence or the “disorder of regulation of alcohol use arising from repeated or continuous use of alcohol” [18] is a form of hedonic indulgence. By consuming alcohol, people are trying to reach well-being by means of hedonia, but because their hedonic needs are not balanced, it only contributes to the maintenance of the drinking habit.
Another factor that apparently contributes to alcohol consumption, dependence, and craving, is low mindfulness [19, 20]. According to mindfulness-to-meaning theory, mindfulness promotes appreciation and savoring of pleasant experiences (hedonia) [21] and re-appraisal of negative events as meaningful life experiences (eudaimonia) [22, 23]. Also, Ryan, Huta, and Deci [6] have established mindfulness as one of the three facets of eudaimonia. Utilizing the healing properties of mindfulness, therapies such as Dialectical Behavior Therapy [24-26], Acceptance and Commitment Therapy [27], Mindfulness Based Stress Reduction [28], Mindfulness-Oriented Recovery Enhancement [29, 30], Mindfulness-Based Relapse Prevention [31-33], and Acceptance-Based Coping for Relapse Prevention [34] intend to manage addictive behaviors or treatment-related discomforts or relapse. Still, the application of mindfulness for enhanced well-being among individuals with alcohol-dependence needs to be explored empirically. Existing interventions contribute to well-being to some extent [35], but often being standalone treatments or focusing on a specific mediating variable, well-being and flourishing outcomes of these interventions are limited. So there is a dire need for development of a novel positive psychology intervention (PPI) to promote well-being of the individuals undergoing treatment for alcohol-dependence that shall also facilitate the ongoing therapies.
1.1. Hedonic Adaptation vs. Eudaimonic Change
Hedonia produces better well-being during a short span, but eudaimonia is dominant in individuals who experience well-being in a long run [36]. Hedonic Adaptation to Positive and Negative Experiences (HAPNE) model of Lyubomirsky & Sheldon suggests that one of the shortcomings of hedonia is hedonic adaptation or the tendency to get adapted to both positive and negative experiences if the stimulation remains relatively static [37]. The allostatic hypothesis proposed by Koob [33], as an extension of the opponent-process theory by Solomon & Corbit [39], emphasizes the narrow division between hedonic homeostasis and hedonic adaptation in alcohol consumption. Initially, there will be a state-a when the consumption of alcohol gives a temporary state of elation. It is followed by state-b with unpleasant sensations experienced slower and longer than state-a [40]. In order to reduce the undesirable experiences, the person will try to go back to the state-a with continued alcohol consumption. This time, due to tolerance or hedonic adaptation, a bit more quantity will be required to reach the same pleasant state. Gradually, this required amount of alcohol will steadily increase, state-b or the unpleasant state will rapidly soar, and an unquenchable craving will take place. State-b will never go back to normalcy or the baseline, unless the alcohol consumption begins [38].
On the other hand, eudaimonia results from virtuous activities – the expression of daimon or the true self – and consequentially, will relentlessly stay active and changing [5, 41]. Mindfulness associated with eudaimonia will also strengthen awareness, alertness, and the ability to recognize numerous changes in the perceptual environment [18]. Apparently, between hedonia and eudaimonia, the latter tends to be a better contributor to the well-being of individuals with addictions.
As the literature suggests, eudaimonic enhancement contributes to better well-being and flourishing of the recipients, but there are not sufficient interventions that aim to enhance eudaimonia for well-being of the individuals with alcohol-dependence that might also facilitate the addiction treatments. Hence, the current study is aimed at the development of a novel intervention, Mindfulness-Based Eudaimonic Enhancement Training (MEET), and estimation of its efficacy as a PPI that promotes well-being and flourishing. This is the first study that tests the efficacy of a novel PPI aimed at eudaimonic enhancement.
The current paper describes the research design and other major elements of the study, elaborates on the intervention and statistical methods adopted, before reporting the results and discussion that explain changes that occurred in the experimental group in comparison with the results of the control group at pre and post intervention conditions. Finally, the conclusions are stated, followed by a brief account of limitations of the study and suggestions for further researches.
1.2. The Present Study
1.2.1. Objectives
The current pilot study was intended to determine the impact of MEET among individuals undergoing treatment for alcohol-dependence, specifically on their mindfulness, eudaimonia, hedonia, and flourishing, by comparing the pre-post test scores of experimental and control groups.
1.2.2. Hypotheses
1) There will not be a significant difference between pre-test scores of experimental and control groups on mindfulness, eudaimonia, hedonia, and flourishing.
2) There will be a significant difference between post-test scores of experimental and control groups on mindfulness, eudaimonia, hedonia, and flourishing.
3) There will be a significant difference between pre-post test scores of the experimental group on mindfulness, eudaimonia, hedonia, and flourishing.
4) There will not be a significant difference between pre-post test scores of control groups on mindfulness, eudaimonia, hedonia, and flourishing.
2. METHODS
2.1. Study Design and Setting
An open trial design was chosen for the administration of MEET where both the researcher and the participants were aware of their participation in the mindfulness-based intervention. However, the details of the expected outcomes of the intervention was debriefed to the experimental group participants after obtaining post-intervention data in order to minimize biased responses.
2.1.1. Procedures
In-patients (N=24) from an Integrated Rehabilitation Centre for Addicts (IRCA) from Thiruvananthapuram district of Kerala, India were recruited. 50% of the participants (N=12) were assigned randomly to the experimental group where they have received MEET along with TaU, while the rest (N=12) were assigned to the control group and received TaU alone. The flowchart of participant recruitment is presented in Fig. (1 and 2). The 30 participants who had fulfilled all eligibility criteria were contacted personally and informed consent was sought to participate in the further study. The participants were informed that they would either receive eight sessions of mindfulness-based intervention as well as administration of the assessment tools twice within a period of 10 days, or they would be asked to respond to the assessments alone. At this point, three participants who did not wish to continue were excluded. From the remaining 27 individuals, 15 were chosen randomly with the help of the website ‘randomizer.org’ [42], and recruited to the experimental group, and 12 to the control group. More participants were included in the experimental group with an anticipated dropout, or absence in two or more sessions.
The pre-intervention data was collected and the intervention was administered by the first author and principal researcher, who holds a post graduation degree in psychology, a mindfulness practitioner for 19 years, and was pursuing doctoral research at the time of the study. The assessment tools and the intervention were administered in the mother tongue of the participants, Malayalam. The researcher had no contact with any of the participants before the administration of the assessments. Session rating at the end of each session was administered by the de-addiction centre staff to minimize experimenter effect. Post-intervention data were obtained by the consultant psychologist at the de-addiction centre, who was blind about the participants’ belongingness to experimental or control groups.
2.1.2. Setting
The whole study was conducted in the de-addiction centre among in-patients enrolled for de-addiction treatment and rehabilitation for 21 to 31 days. TaU at the IRCA centre included pharmacotherapy and counselling or psychotherapy for the in-patients and accompanying family members. Besides, they were provided with training on management of craving and withdrawal symptoms. The in-patients could opt to participate in recreational activities, play indoor/ outdoor games, workout at the gym, or practice yoga.
2.1.3. Inclusion Criteria
Diagnosis of alcohol-dependence; age between 23 and 70; educational qualification at least 10th grade (pass or fail); completed at least seven days of treatment for alcohol-dependence and at least 10 remaining days of treatment at the time of the initiation of intervention; low eudaimonia (score <40) according to the Questionnaire for Eudaimonic Well-Being (QEWB).
2.1.4. Exclusion Criteria
Current diagnosis or previous history of psychotic disorder; co-morbid chronic illnesses/ other addictions; depressive symptoms; suicidal ideation; potential withdrawal risk.
Individuals with current or previous diagnosis of psychotic disorders were excluded [43, 44]. Although mindfulness is found to be not harmful, the possibility of minor harms to a minority was taken into consideration resulted in this pre-caution [45]. Individuals with co-morbid chronic illnesses or addictive disorders other than alcohol-dependence were also excluded because their illness might act as an extraneous variable, affecting the homogeneity of the groups. For instance, heavy smoking often results in breathing difficulties that require special attention during mindful breathing exercises. Depressive symptoms and suicidal ideation are other conditions that could be contra-indication to mindfulness meditation practice, and hence, individuals with the same were excluded [46, 47]. Finally, considering the history of withdrawal from previous training/ therapy/ counselling sessions, individuals with potential withdrawal risk were identified and excluded.
2.2. Participants
The characteristics of the participants are presented in Table 1. The study consists entirely of male participants because no females had volunteered to participate in the study. Out of the 15 participants who were initially assigned to the experimental group, three individuals who had missed two or more sessions were excluded and the remaining 12 are included in the current study. All the participants were diagnosed with alcohol-dependence according to ICD-11 criteria by a clinical psychologist at the de-addiction centre. Participant selection was made with the help of the de-addiction centre staff who had filtered out individuals who had met the exclusion criteria. Experimental and control groups did not differ significantly based on the number of treatment days completed and remaining. None of the participants had previous experience with mindfulness or any kind of meditation.

| Demographics | Group I (N=12) | Group II (N=12) | |
|---|---|---|---|
| - | (N%) | (N%) | |
| Gender | Male | 12 (100) | 12 (100) |
| Education | - | - | - |
| 10th or less | 5 (42) | 4 (33) | |
| 12th | 5 (42) | 7 (58) | |
| Graduation/Diploma | 2 (16) | 1 (9) | |
| Marital status | - | - | - |
| Unmarried | 6 (50) | 7 (58) | |
| Married | 6 (50) | 5 (42) | |
| Place of residence | - | - | - |
| Rural | 9 (75) | 8 (67) | |
| Semi-urban | 1 (8) | 3 (25) | |
| Urban | 2 (17) | 1 (8) | |
| Income | - | - | - |
| Below 10,000 | 1 (8) | 2 (17) | |
| 10,001 – 30,000 | 6 (50) | 7 (58) | |
| 30,001 – 60,000 | 4 (34) | 2 (17) | |
| 60,001 – 1,00,000 | 1 (8) | 1 (8) | |
| Age group | - | - | - |
| Below 30 | 1 (8) | 2 (17) | |
| 31-50 | 8 (67) | 8 (66) | |
| 51-70 | 3 (25) | 2 (17) | |
| Occupation | - | - | - |
| Daily wages | 7 (58) | 9 (75) | |
| Private sector | 4 (33) | 1 (9) | |
| Self-employed | 1 (9) | 2 (16) | |
2.3. Measures
2.3.1. Five-Facet Mindfulness Questionnaire (FFMQ)
Is a short 15-item version of the original 39-item FFMQ published by Baer et al. [48]. The five facets of mindfulness being assessed through this tool are – i) observing, ii) describing, iii) acting with awareness, iv) non-judging of inner experience, and v) non-reactivity to inner experience [49]. FFMQ gives instances of mindfulness in daily life and ask to rate it on a five-point scale where 1 indicates ‘never or very rarely true’ and 5 indicates ‘very often or always true’. The short version’s factor structure resembles that of the original version, and the internal consistency of the 15-item FFMQ is between .64 and .83 [50]. Administered in the Indian population, 39-item FFMQ has shown internal consistency reliability between .72 to .92 [51]. Another study conducted in Kerala, India, has reported that the factor structure of the 15-item version was consistent when compared to the 39-item version [52]. The current study has estimated Cronbach’s alpha of FFMQ-15 as between .71 and .77.
2.3.2. Questionnaire for eudaimonic well-being (QEWB)
Contains six domains of eudaimonia: i) self-discovery, ii) perceived development of one’s best potentials, iii) a sense of purpose and meaning in life, iv) intense involvement in activities, v) investment of significant effort, and vi) enjoyment of activities as personally expressive. Consisted of 21 items QEWB employs a five-point Likert scale that ranges from 0 to 4, where 0 being ‘strongly disagree’ and 4 being ‘strongly agree’. It also instructs the recipient to report what they feel is actually going on, rather than what they wish things to be. Seven items in QEWB are reverse scored. It has high internal consistency, convergent validity, construct validity, and incremental validity [53]. Areepattamannil & Hashim [54] have tested the psychometric properties of QEWB among an adolescent population in Kerala, India. They have found that QEWB’s internal consistency reliability (Cronbach’s alpha) was .87, convergent validity .73 and .69, and construct validity .60 and -.65. The current study observed the Cronbach’s alpha of QEWB as ranging between .83 and .85.
2.3.3. Positive and Negative Affect Scale (PANAS)
Is a commonly used tool to assess hedonia [55, 56] consisted of two subscales with 10-item each for positive and negative affect. Only the positive affect scale is used in the current study as a measure of hedonia. PANAS assesses the perceived affect of the individual in the past week, using a five-point scale ranging from 1 to 5, where 1 indicates ‘very slightly or not at all’ and 5 indicates ‘extremely’. The minimum possible score for positive affect is 10 and the maximum, 50. PANAS has high internal consistency, adequate convergent validity and discriminant validity [57]. Applied among an Indian population, PANAS as a whole, had Cronbach’s alpha of .90 and .96 for the 10-item positive affect subscale. Also, the convergent validity of positive affect subscale was .95 [58]. In the current study, Cronbach’s alpha of the positive affect sub-scale of PANAS was .84 to .85.
2.3.4. Flourishing Scale (FS)
Is an eight-item scale that was used to assess flourishing that includes the aspects of ‘positive relationships, feeling of competence, and meaning and purpose in life’. Assessed using a seven-point scale where 1 indicates strong disagreement and 7 represents strong agreement; its higher score signifies high flourishing. The scale has good internal reliability [59]. When administered among Indian population, FS was reported to have shown Cronbach’s alpha of .80, .85, and .91 [60]. In the current study, FS showed Cronbach’s alpha that ranged from .76 to .90.
2.4. Intervention
Tailored exclusively for the needs of individuals undergoing treatment for alcohol-dependence, MEET contains eight sessions that intend to promote specific aspects of eudaimonia as proposed by Waterman et al. [53] – self-discovery, development of one’s actual potentials, a sense of meaning and purpose in life, absolute engagement in activities, increased ability to invest effort in activities for self-development, and enjoyment of those activities – through mindfulness. Attempts to develop mindful awareness through seven sensory modalities – i) vision, ii) audition, iii) taction, iv) olfaction, v) gestation, vi) kinesthesia, and vii) proprioception – is one of the major contribution of MEET. It combines both formal and informal mindfulness practices, giving priority to the latter anticipating that the participants would continue to apply mindfulness in daily life with or without the deeper, formal, practice. Participants are trained to be conscious of the sensory, cognitive, and affective elements of the awareness spectrum. MEET utilizes real stimuli for sensory experience, guided imagery, instructions to observe thoughts and emotions, and probing to encourage recipients to share their experiences for better self-awareness. Themes covered in each session are described in Table 2.
Based on the literature about the characteristics of individuals with alcohol-dependence in India [61-65], and also considering the suggestions by experts in de-addiction, the intervention protocol was prepared in a simple and easy-to-understand manner, prioritizing the convenience of the recipients. The initial draft of the intervention protocol was modified considerably after receiving expert opinion from psychologists working with individuals undergoing treatment for alcohol dependence. The second draft was distributed among five experts from the fields of mindfulness and de-addiction. The eight sessions of MEET were rated by the experts in a five-point scale based on their adequacy, theoretical soundness, effectiveness as a mindfulness tool, and effectiveness as a eudaimonic enhancement technique. Further, major elements of each session were rated based on their adequacy and relevance. The feedback from the experts supported the application of MEET among the target population in the form of a pilot study.
As part of the pilot study, MEET was administered to a group of maximum eight participants for eight consecutive days. The gaps between sessions were avoided due to the short duration of inpatients’ stay at the de-addiction centre. A session was for one hour daily, recognizing the inability of the participants to stay focused for a long time, primarily due to the effect of ongoing de-addiction treatments. The sessions were conducted at the de-addiction centre, in an enclosed room to avoid extraneous disturbances and to ensure privacy, with openings to the surrounding greenery, where nobody except the participants and the researcher was present. The pre-intervention data were collected one to three days before initiation of the intervention and the post-intervention data were collected the next day after the completion of the intervention.
| Sessions | Theme | Formal Practices |
|---|---|---|
| One | Introduction | Mindful breathing |
| Two | Wilderness – getting close to nature | Mindful breathing |
| Three | Trees & rain – gratitude | Mindful breathing |
| Four | Flowers – loving-kindness & compassion | Raisin exercise, mindful breathing |
| Five | Mountains – hope, resilience, perseverance & abstinence | Mindful walk, mountain meditation, mindful breathing |
| Six | Positive relationships – empathy, happiness, contentment & meaning in life | Body scan, mindful breathing |
| Seven | The universe, a wider perspective –daimon, flow, vitality & being alive | Mountain meditation, mindful walk |
| Eight | The passing time – sun at different times of the day, seasonal changes & life cycles | The time meditation, lake meditation, mindful breathing |
2.5. Statistical Analysis
Data were analyzed using IBM SPSS software to explore the characteristics of the data, and to test the hypotheses.
2.5.1. Shapiro-Wilk Test
To determine the normality distribution of the baseline data in order to choose suitable statistical tools for hypotheses testing, a test of normality was conducted. Shapiro-Wilk test was employed as a test of normality. The test was adopted due to its utility in testing small samples [66].
2.5.2. Independent-Sample t-test
On account of the results of Shapiro-Wilk test indicating normal distribution of the data, parametric tests were adopted to compare the means of pre and post scores of experimental and control groups. Independent sample student’s t test was used to test hypotheses 1 and 2. Independent sample t-test is used when the groups of data are not dependent on each other but comes from unique and independent respondents [67, 68]. The test was used to determine whether the mean scores of the respondents from the control and experimental groups were significantly different or not.
2.5.3. Paired Sample t-test
Paired sample student’s t-test was employed to test hypotheses 3 and 4. Paired sample or dependent sample or repeated measure t-test is used to compare the means of two datasets from the same individual taken at different times, or conditions [69]. The pre-post test scores of experimental group as well as control group were compared using paired sample t-test.
2.6. Ethics Approval and Consent to Participate
This study was approved by the Department of Psychology, School of Social and Behavioral Sciences, Central University of Karnataka, India (Ethical clearance number: CUK/SDBD/Psy/EC-11/2019-20/11, Dated 03-01-2020). Informed consent was obtained from the participants before initiation of the study and the experimental group was debriefed about the expected outcome after the administration of post-intervention assessment battery.
3. RESULTS
The baseline data were tested for normality by using Shapiro-Wilk test. The results showed normal distribution for the pre-intervention experimental group’s scores on eudaimonia (W=.935, p=.430), mindfulness (W=.932, p=.406), hedonia (W=.931, p=.396), and flourishing (W=.876, p=.079). The results of post-intervention experimental group were found to be normally distributed based on the scores of eudaimonia (W=.980, p=.982), mindfulness (W=.917, p=.263), hedonia (W=.951, p=.654), and flourishing (.921, p=.290). The baseline assessment of control group was also normally distributed as indicated by the results on eudaimonia (W=.922, p=.299), mindfulness (W=.910, p=.211), hedonia (W=.978, p=.972), and flourishing (.954, p=.701). Finally, the post-intervention assessment among the control group was also found to be normally distributed as revealed by the results on eudaimonia (W=.869, p=.063), hedonia (W=.946, p=.575), and flourishing (W=.928, p=.357). The result also revealed the sample was not normality distributed based on the scores of mindfulness (W=.836, p=.025). Further explorations with descriptive statistics revealed the presence of an outlier in the post-intervention control group data. The researchers have opted for parametric tests for all conditions, after considering the outlier in the post-intervention control group being a high scorer on mindfulness, reducing but not significantly affecting the mean difference between conditions and thus not contributing to erroneous acceptance or rejection of the hypotheses.
(Tables 3-6) show the results of testing hypotheses 1, 2, 3, and 4, respectively. The null hypothesis stating the non-significant difference between pre-test scores of experimental groups on mindfulness, eudaimonia, hedonia, and flourishing is accepted. Hypothesis stating the significant difference between post-test scores of experimental and control groups on mindfulness, eudaimonia, hedonia, and flourishing is partially accepted, with the exception of hedonia being not significantly different. Hypothesis stating the significant difference between pre-post scores of experimental group was accepted, confirming the effect of intervention on the experimental group. Finally, the null hypothesis stating that there will not be a significant difference between pre-post scores of control group on mindfulness, eudaimonia, hedonia, and flourishing is partially accepted, with the exception of hedonia and flourishing being significantly different. Moreover, flourishing was significantly higher in post-intervention experimental group when compared to post-intervention control group. The following is the summary of the results based on the outcome measures.
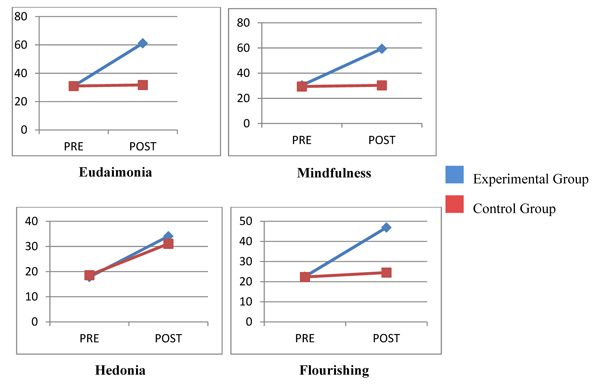
3.1. Changes in Mindfulness
Table 3 shows the independent-sample t-test results of experimental and control groups, displaying the mean and SD. The result indicated the homogeneity between groups on mindfulness before administration of MEET. And Table 4 shows the mean and SD of the scores of experimental and control groups after intervention, and substantiated the significant difference with large effect size. Table 5 shows the pre and post tests comparison of experimental group where the significant difference is present with an effect size as large as before. On the other hand, Table 6 shows the pre-test post-test comparison of control group where no significant difference was found. The result indicates the noteworthy rise in mindfulness after exposure to MEET.
3.2. Changes in Eudaimonia
The mean scores of experimental and control groups at pre-intervention stage on eudaimonia do not have a significant difference but after intervention the experimental group has reported nearly twice eudaimonic well-being score in comparison with the control group. Experimental group has also shown significantly higher eudaimonia with large effect size post-intervention, whereas control group has reported no significant improvement.
| Variable | Experimental | Control | t | p | ||
| - | Mean | SD | Mean | SD | - | - |
| Eudaimonia | 31 | 6.13 | 31 | 5.79 | 0 | 1 |
| Mindfulness | 30.33 | 4.61 | 29.41 | 5.12 | 0.46 | 0.65 |
| Hedonia | 17.83 | 3.99 | 18.58 | 3.75 | 0.47 | 0.64 |
| Flourishing | 22.5 | 6.51 | 22.33 | 3.93 | 0.07 | 0.94 |
| Variable | Experimental | Control | t | p | Cohen’s d | Glass’s Delta | ||
| - | Mean | SD | Mean | SD | - | - | ||
| Eudaimonia | 61.1667 | 7.69691 | 31.75 | 4.57513 | 11.381 | 0 | 4.64613 | 6.4297 |
| Mindfulness | 59.4167 | 3.98767 | 30.3333 | 5.03322 | 15.689 | 0 | 6.40513 | 5.77829 |
| Hedonia | 34.0833 | 3.94181 | 31.0833 | 5.07146 | 1.618 | 120 | 0.66052 | 0.59155 |
| Flourishing | 46.9167 | 4.87029 | 24.5 | 3.96576 | 12.364 | 0 | 5.04754 | 5.65256 |
| Variable | Pre-test | Post-test | t | p | Cohen’s d | ||
| Mean | SD | Mean | SD | - | - | - | |
| Eudaimonia | 31 | 6.13485 | 61.1667 | 7.69691 | 15.382 | 0 | 4.44 |
| Mindfulness | 30.3333 | 4.6188 | 59.4167 | 3.98767 | 19.658 | 0 | 5.676 |
| Hedonia | 17.8333 | 3.99621 | 34.0833 | 3.94181 | 17.316 | 0 | 5.001 |
| Flourishing | 22.5 | 6.51572 | 46.9167 | 4.87029 | 17.367 | 0 | 5.014 |
| Variable | Pre-test | Post-test | t | p | ||
| - | Mean | SD | Mean | SD | - | - |
| Eudaimonia | 31 | 5.79 | 31.75 | 4.57 | 0.76 | 0.459 |
| Mindfulness | 29.41 | 5.12 | 30.33 | 5.03 | 1.28 | 0.224 |
| Hedonia | 18.58 | 3.75 | 31.08 | 5.07 | 0.21 | 0 |
| Flourishing | 22.33 | 3.93 | 24.5 | 3.96 | 3.02 | 0.012 |
3.3. Changes in Hedonia
At baseline, both groups have shown similar amount of hedonia, as Tables 3 suggests, with control group showing a slightly higher but not statistically significant mean. After the intervention, both experimental and control groups have reported better hedonia, and experimental group has obtained slightly better hedonia though the difference is not significant. Experimental as well as control groups reported significant elevation in hedonia after intervention when compared to the pre-intervention state of the respective groups, but experimental group has larger mean difference. Overall, the results indicate the impact of both MEET and TaU on enhancing eudaimonic well-being.
3.4. Changes in Flourishing
Experimental and control groups scored nearly the same mean for flourishing prior to the intervention, but after administration of MEET, the groups reported a significant difference. Experimental group has higher score with large effect size. As it can be assumed, experimental group also showed significant difference with large effect size when pre-post scores were compared. There is a significant difference between pre-post mean scores of control group at 0.05 level, but the difference is not as big as that of the experimental group.
4. DISCUSSION
The current pilot study was carried out to assess the feasibility of the research design, study tools administered, and the implementation of the novel intervention, MEET. The study was aimed at estimating the efficacy of MEET in enhancing mindfulness, eudaimonia, hedonia, general well-being, and flourishing of the individuals undergoing treatment for alcohol dependence.
Homogeneity between experimental and control groups at the baseline level was verified by comparing the pre-intervention mean scores. Following intervention, compared to the active control group, experimental group reported significantly higher eudaimonia, mindfulness, and flourishing. An analysis of effect size was done to determine the extent of the impact of the intervention on experimental group. The results indicate that eudaimonia has the largest effect size, followed by mindfulness, and flourishing. For hedonia, effect size is large but comparatively smaller than the other variables. Ialongo [70] described that it is appropriate to use Cohen’s d when the groups share similar sample size and variance, regardless of the sample size; but it is better to use Glass’s delta when the SD greatly differs in an independent-sample t-test. Hence, both results are reported here which do not differ considerably. Overall, these results clearly demonstrate the combined effect of TaU and MEET as superior to the use of TaU alone.
The results indicate the impact of MEET on mindfulness, eudaimonia, hedonia, and flourishing, pointing out its efficacy as a PPI. One of the explanations for the large effect sizes in the current pilot RCT is the use of the intervention, developed based on the concepts adopted by the assessment tools administered. Cheung & Slavin [71] reported that the “experimenter-made” interventions developed for the target population yield effect sizes twice as large as other adopted interventions. Moreover, the formal techniques used in the intervention are adopted from previous literature on mindfulness-based interventions, particularly MBSR [72], found to be effective for both clinical and positive outcomes [28, 73]. Considering that the individuals are undergoing de-toxification as well as pharmacological and psychological therapies to manage symptoms of alcohol-dependence, craving, and related difficulties, long durations of formal practices were avoided and informal practices were introduced with priority given to the direct application of the same to daily life situations. The results confirmed previous studies, including that of Birtwell et al. [74] and Hanley et al. [75], in which it was found that informal mindfulness practices are apparently effective in better health and well-being. Moreover, the reappraisal of positive and negative experiences were incorporated in MEET, along with guidance to focus on savoring of pleasant experiences, which are also reported earlier as mediators between informal mindfulness practice and well-being [76]. A significant improvement in hedonia and well-being was also found. It supports the studies by Howells et al. [77] and Malboeuf-Hurtubise et al. [78] who found that mindfulness-based interventions improved well-being, particularly hedonia. Finally, Bakker et al. [79] point out that the effect sizes of studies with small samples should be dealt with caution, but regardless of the magnitude of the effect, the results suggest a significant impact of the intervention under the specified context.
There is significant difference between mean scores of experimental group on eudaimonia, mindfulness, hedonia, and flourishing, before and after the intervention. Along with the results previously described, it shows a definitive efficacy of MEET. The interaction of the variables, process of changes that occurred, effectiveness rather than efficacy of the intervention, and the mechanisms behind the intervention effectiveness are to be studied further.
Pre-post tests of control group suggest that TaU did not benefit the mindfulness and eudaimonia of the participants. There is a significant improvement in flourishing, though further studies are required to know how long the effects will last. One possibility of the significant improvement in flourishing with no similar effect observed in eudaimonia is that, flourishing was assessed in terms of subjective feelings or perceptions about oneself, e.g. “I am optimistic about my future”, that might be influenced by positive variables such as hope, self-efficacy, self-love, optimism, and motivation to strive for a better future. On the other hand, eudaimonia represents both objective and subjective aspects that reflect not only the person’s hopes and perceptions, but also a true account of what the person is willing to be [53].
The current result shows that TaU contributes to hedonic well-being, that is highly dependent on external circumstances and physical/ tangible contributors. If it is the same happened with TaU, it is highly likely that the impact will gradually diminish once the individuals are out of therapy and rehabilitation, unless internal motivation to abstain or adoption of adaptive drinking patterns sustain.
Experimental and control groups differ significantly in the mean scores of mindfulness, eudaimonia, and flourishing emphasizing the impact of MEET. Regarding hedonia, MEET and TaU have produced nearly the same effect, MEET showing slightly higher scores. The results show promising impact on well-being, mindfulness, and eudaimonia that could prevent relapse by helping the individuals to manage consumption of alcohol after completion of the treatment and medications.
The novel mindfulness-based intervention shows significant efficacy as a PPI, with notable impact on eudaimonic well-being. It needs to be mentioned here that the large effect sizes should not be misleading, and the characteristics of sample populations should also be considered before assuming the potential effectiveness of MEET on basis of its reported efficacy. Save for the limited sample size, the study has also included the participants based on their level of eudaimonia, which might have resulted in a significant change after the intervention that was specifically focusing on eudaimonic enhancement. A deficiency in eudaimonia also denotes the need for eudaimonia resulted from perceived scarcity, indicating an orientation toward eudaimonia. This inclination of the participants was evidently addressed by the intervention that had contributed to the inflated eudaimonia and associated positive variables.
Another key factor that has a predominant role on current results is the duration of the intervention. Unlike the usual once-a-week sessions of mindfulness-based interventions, MEET has eight sessions on consecutive days. This immediate change in the reported scores of eudaimonia and related factors is mostly contributed by the peculiar features of the population under study. Those individuals undergoing rehabilitated addiction treatment were attending several therapies, counselling, and psycho-education programs, and were probably in a state of receptiveness and openness to positive changes. Further, addiction is a result of a desperate attempt to elevate well-being, and the same was the sole focus of MEET. So, it is likely that when they were introduced to new ways of finding meaningful happiness, they recognized it as better than pleasure alone, and quickly began to explore these novel routes to well-being.
Finally, the sessions were shortened to one hour per day, taking heed of the physical and psychological state of in-patients at the de-addiction centers. It was beyond their ability to focus on any task for long durations and they tended to get drowsy, fatigued, or exhausted occasionally. In addition, they were unable to read or write much and too distracted to practice formal meditations. Thus, all mandatory and/or formal meditation practices were excluded and instead, they were trained to focus on and cater to the sensory, cognitive, and affective needs from daily activities. Further studies shall throw more light on explaining the reasons for intervention efficacy when these constraints were present. The long-term impact of the MEET shall also be studied further.
CONCLUSION
The study emphasizes the potential efficacy of the novel intervention MEET for enhancement of the positive functioning of individuals undergoing treatment for alcohol-dependence. The study accentuates the need for PPIs in clinical settings, the response of clinical population to well-being interventions, the role of mindfulness on enhancement of hedonic and eudaimonic well-being, and the utility of a mindfulness-based intervention as a PPI. Despite the limitations, the current pilot RCT recounts the possible advantages of the intervention and suggests further studies in the direction of positive psychology, mindfulness, and eudaimonic enhancement. Finally, the current pilot study denotes the feasibility of the study design, utilization of the research tools, and application of MEET among individuals undergoing treatment for alcohol dependence in Kerala, India. Based on the current study results, the main study or similar future studies shall be conducted to explore the impact of MEET on alcohol-dependence treatment and relapse-prevention, considering the suggested changes for improvement.
LIMITATIONS AND SUGGESTIONS
Although the study reports high impact of MEET as a PPI among individuals with alcohol-dependence, the statistical data should be dealt cautiously, due to the small sample size. Being a pilot trial to find the efficacy of a novel intervention among a specific clinical population where several possible extraneous and confounding variables are controlled, the sample size has become too low. The main study followed by the current pilot study, or further future studies shall adopt large sample sizes. Bigger samples will also allow the applications of more statistical techniques to interpret the data. Additionally, it is recommended to add a placebo group to confirm the effectiveness of the group, apart from a control group that did not receive any intervention other than TaU.
The population consists entirely of men and the efficacy of the intervention among women is non-represented. It is also recommended to study the efficiency of the intervention in real-life contexts, and also its impact in the long-run. Follow-up studies are essential to assume the long-term efficacy of MEET, particularly its role in facilitating TaU and relapse prevention.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Department of Psychology, School of Social and Behavioral Sciences, Central University of Karnataka, India (Ethical clearance number:CUK/SDBD/Psy/EC-11/2019-20/11, Dated 03-01-2020).
HUMAN AND ANIMAL RIGHTS
No Animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from the participants before initiation of the study and the experimental group was debriefed about the expected outcome after the administration of post-intervention assessment battery.
AVAILABILITY OF DATA AND MATERIALS
The datasets generated during and/or analyzed during the current study are available from the corresponding author [A.J.G] on reasonable request.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

