All published articles of this journal are available on ScienceDirect.

Effect of A Resilience Programme Through Group Dynamics on the Academic Problems of Grade 7 Students, Chiang Mai University Demonstration School
Abstract
Background:
Early adolescents may encounter adverse situations that could cause stress and anxiety. To prevent mental health problems and promote mental health, resilience should be promoted in early adolescents.
Objectives:
The objectives of this study were to develop a resilience program and evaluate the effectiveness of such a programme on the academic problems of Grade 7 students of the Chiang Mai University Demonstration School, Chiang Mai, Thailand.
Methods:
This quantitative research used a quasi-experimental design, which was a controlled study with a pretest and post-test. The purposive selection was used to choose 70 participants from the Grade 7 students, the academic year 2021 from the Chiang Mai University Demonstration School. The criteria were students who had the lowest resilience inventory score from the student population. The participants were classified with stratified random sampling into the experimental groups (n=35), who received a resilience program through the group’s dynamics once a week for 11 weeks at 60 minutes each time, and the control groups (n=35), who received a resilience knowledge sheet and had a normal life. Two participants in each group withdrew, leaving a total of 33 participants per group. The data were collected by assessing before and after participating in the programme with a general information questionnaire, the Canadian Occupational Performance Measures (COPM), and Resilience Inventory. Descriptive statistical analysis, an independent t-test, and paired t-test were used to analyse the data.
Results:
This resilience programme had an overall consistency index of 0.78. After treatment, the experimental group and control group had a statistically significant difference in the pretest and post-test resilience scores. (p < 0.01 and p < 0.05). The experimental group had pretest and post-test significant differences in academic performance and satisfaction (p < 0.01), while the control group had no statistically significant difference. There was a statistically significant difference in the post-test academic satisfaction between both groups. (p < 0.01), while academic performance displayed no statistically significant difference.
Conclusion:
This resilience programme, through the groups’ dynamics could contribute to the resilience, academic performance, and academic satisfaction on academic problems.
1. INTRODUCTION
Early adolescence is the changing phase of life from middle childhood to adolescence in which the individual is aged between 10 to 15 years. People also experience rapid physical, cognitive, emotional, and psychosocial growth [1]. Grade 7 students are early adolescents who have changed from elementary to junior high school. They have rapid physical growth, which affects their self-image, and they need independence in their life and acceptance from society [1]. Early adolescence learning is also a result of participation in various occupations, which the most important occupation for this age is education. Education has activities needed for learning and participating in the educational contexts [2]. Furthermore, early adolescents could encounter challenges and academic problems that could cause stress and anxiety [3]. These include academic problems; such as academic pressure, workloads during online education, division of the study, etc. To prevent mental health problems, reduce the severity of facing adverse situations, promote the ability to participate in activities, and promote mental health, resilience should be promoted in early adolescents. Resilience helps people effectively face stressful and adverse situations in their life [4-7]. Previous studies found that resilient students could cope with challenging situations and academic pressure effectively. Moreover, resilience could predict the student’s academic performance, self-esteem, life satisfaction and lead to well-being [8-10].
Resilience can contribute to four levels: individual, family, school, and community [11]. Resilience has three components that consist of “I have”, “I am”, and “I can”. “I have” infers external support factors of people, such as, having good role models, a trusting relationship with others, freedom, health, education, welfare, and safety services. “I am” infers a person realizes about themselves; such as, self-esteem, self-identity, self-responsibility, and self-confidence. “I can” infers that the individual realizes their abilities through interaction with other people; such as, communication, problem-solving, interpersonal, and emotional skills [6].
From the literature review, resilience was strengthened using cognitive behavioral therapy (CBT), acceptance and commitment therapy (ACT), and Grotberg's resilience concept through the individual and group. The CBT focused on understanding and adjusting automatic thoughts. The CBT was used for clinical treatment for adolescents; such as depression [12] and adolescents at high risk from parents with alcohol dependence [13]. The duration of the programme was once a day for eight consecutive days for 50 minutes each time [14], and once a week for 10 weeks for 50 minutes each time [13]. The ACT was applied in the resilience programme, which emphasized understanding, acceptance, and the present. This helped people to face adversity consciously. The duration of the programme was once a week for eight weeks for 60 to 90 minutes each time [15], and 11 sessions for two hours per session [16]. Additionally, a systematic review showed that the CBT and mindfulness training was effective in promoting resilience. The combination of the two treatment approaches had a positive effect on resilience at the individual level. The duration of the programme was varied ranging from one session of two hours to multiple sessions totaling 28 hours, with most sessions being 60 to 90 minutes each for several weeks. Thus, this was the right time for a person to learn and develop new skills [17]. From all the above, the CBT and ACT have been effective in promoting resilience in early adolescents. Most resilience programmes were conducted in group activities because early adolescents seek self-identity and social acceptance. Group dynamics also helped individuals learn and develop themselves through interactions with others, as this promoted trust and cooperation in therapy [18]. In occupational therapy, group dynamics not only encouraged learning and interaction, but also helped to develop the role of individuals in group collaboration [19].
From previous studies, it could be seen that the resilience programme was developed by applying the CBT, ACT, or combining both approaches for adults in the workplace. However, the ACT in resilience programmes had never been applied to early adolescents in Thailand. Thus, the researchers focused on developing a resilience programme based on Grotberg’s resilience concept [6], CBT [20, 21], and ACT [22, 23] through Cole’s seven-step model of group dynamics [19]. The duration of this programme was once a week for 11 weeks at 60 minutes each time. This present study focused on developing a resilience programme for Grade 7 students of the Chiang Mai University Demonstration School because all students had to pass the foundation academic knowledge test. As such, they had to adapt themselves to a new educational environment; for example, institutions, learning, teachers, staff, friends, etc. All students were assorted by Thai consonant names, consequently resulting in each classroom having assorted students with diverse learning abilities. In addition, some students had to relocate from their home to live in dormitories, which caused students having to adjust. From all the above, the researchers aimed to develop a resilience programme and evaluate the effect of the programme on the academic problems of Grade 7 students of Chiang Mai University Demonstration School.
2. MATERIALS AND METHODS
2.1. Sample Size and Sampling Technique
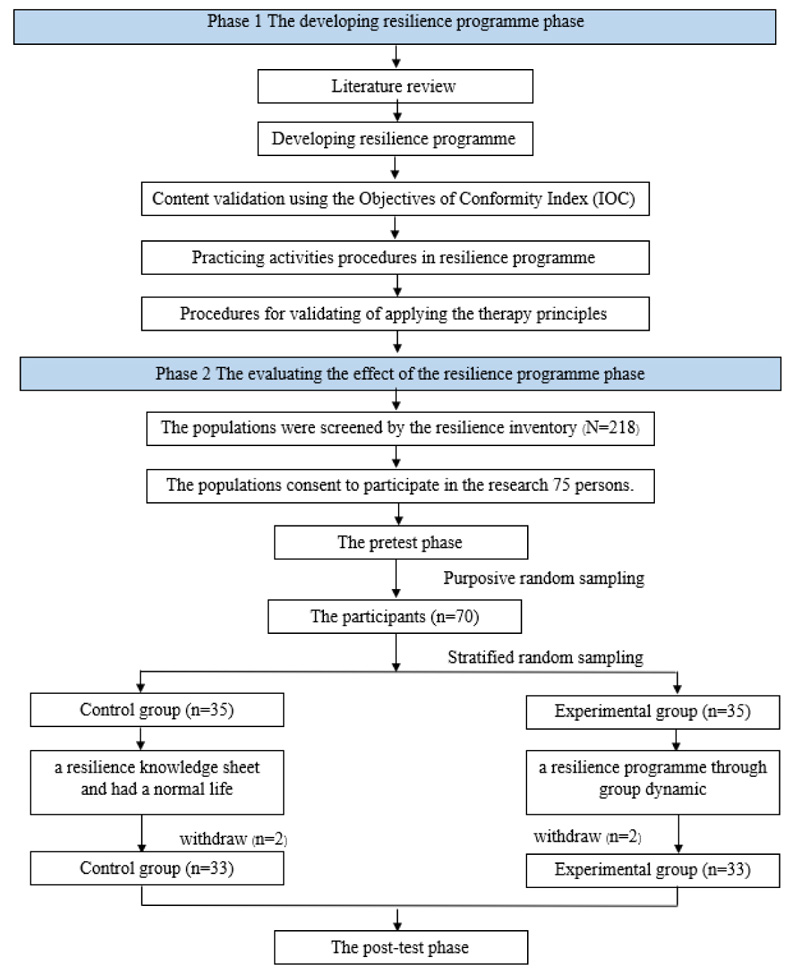
This quantitative research used a quasi-experimental design, which was a controlled study with a pretest and post-test. The population in this study comprised Grade 7 students in the academic year 2021 from Chiang Mai University Demonstration School, Chiang Mai, Thailand. The researchers determined the sample size from the G*Power 3.1 test power analysis by using the raw data from previous studies related to the CBT, ACT, and Grotberg’s resilience concept in adolescents. The sample size was determined by .80 statistical power with a 95% confidence level. The effect size was between 0.8430552 [ 24 ] to 1.956211 [ 25 ] with a total of 66 participants. To prevent volunteers withdrawing from this study, the researchers assigned a total of 70 participants. Purposive selection was used to choose 70 participants who had the lowest resilience inventory score because the researchers aimed to evaluate the effect of a resilience programme in promoting resilience in Grade 7 students. The participants were divided by stratified random sampling into the experiment group and control group with a total of 35 students in each group. The researchers determined the characteristics of the control group and the experimental group to be the most similar; such as, gender, resilience, family’s socio-economic status, residential style, parents’ marital status, family relationship, and grade point average. Two people in each group withdrew leaving a total of 33 participants per group.
2.2. Data Collection Tools
The data were collected by using three tools: a general information questionnaire, Canadian Occupational Performance Measures (COPM), and Resilience Inventory.
(1) The general information questionnaire collected the data about gender, family’s socio-economic status, average monthly income per household, residential style, parents’ marital status, family relationship, and grade point average.
(2) The COPM measured the personal occupational performance and satisfaction, which the participants rated the score by themselves [26]. This measurement’s psychiatric properties were in terms of test-retest reliability (r = 0.842) [27], convergent validity that assessed occupational performance, responsiveness, the reliability in occupational performance was 0.95, occupational satisfaction was 0.93, and the total was 0.97 [28]. A semi-structured interview was used to collect the data, which comprised five steps: 1. Specified the academic problems, 2. determined the priority of the academic problems, and 3. rated the academic performance and academic satisfaction scores. Scores ranged from 1 point, which was the lowest, to 10 points. The performance score (PS1) was calculated from the sum of the academic performance scores divided by the number of problems, and the satisfaction score (SS1) was calculated from the sum of the academic satisfaction scores divided by the number of problems. 4. Retest: After the treatment, the participants had to rate the academic performance scores (PS2) and academic satisfaction scores (SS2). This retest score showed the changes of the improved academic performance and satisfaction on academic problems. It could be calculated from PS2-PS1, and the changes of academic satisfaction were calculated from SS2-SS1, and 5. the follow-up procedures [29].
(3) Resilience Inventory was used to measure the resilience score. This inventory was developed based on Grotberg’s resilience concepts. This inventory investigated the reliability in university students, Cronbach’s alpha coefficient was .86 - .91. and there was structural validity. The inventory had 28 questions related to three resilience components. Resilience Inventory used a five-point Likert scale where 1 = strongly disagree, 2 = disagree, 3 = indifference, 4 = agree, and 5 = strongly agree. The participants had to choose a choice to answer each question that reflected their level of opinion on that question. The resilience score could be interpreted from the sum of the level of opinion with a score ranging from 28 (the lowest score) to 140 (the highest score). It could interpret that the students who had a high sum of resilience score had high resilience, whereas the students who had a low sum of resilience had low resilience [11].
2.3. Research Procedure
The research procedure consisted of two phases as follows:
Phase 1. Developing the resilience programme: The researchers reviewed the literature, and the research proposal was approved by the Ethics Committee, Faculty of Associated Medical Sciences, Chiang Mai University, Thailand. The researchers participated in the cognitive and behavioural psychotherapy workshop for student mental health care organised by the Cognitive Behavioural Therapy Alliance of Thailand (CAT). The resilience programme was verified for the content validity using the index of item-objective congruence (IOC) by a mental health occupational therapist, a mental health occupational therapy instructor, an instructor in educational psychology and guidance, an educational psychology and guidance specialist, and a child and adolescent psychiatrist. The specialists had to be qualified with at least 10 years of mental health and psychology work experience, have knowledge about the CBT, ACT, and group dynamics. After verifying the resilience programme, the researchers and research assistant practiced the procedures of the activities with other participants similar to the study participants. Then, the certificated cognitive behavioural psychotherapist verified the validity of applying the therapy principles. Based on the therapist's recommendations, the researchers revised the programme’s details.
Phase 2. Evaluating the effect of the resilience programme: The population was screened by the resilience inventory. In the pretest phase, the participants completed the general information in the Google Form and were interviewed about their academic problems using the COPM. The experimental group had acquired the resilience programme through the group’s dynamics (Table 1), while the control group received a resilience knowledge sheet and had a normal life. In the post-test phase, the participants undertook the Resilience Inventory and the COPM to follow-up on the effectiveness of the programme. The duration of the study was from September to November 2021.
The details of the resilience programme are shown in
Table 1.
The data collection procedure is shown in Fig. (1) .
| Title | Particulars |
|---|---|
| Conceptual framework | 1. Grotberg’s resilience concept [6] 2. Cognitive behavioural therapy (CBT) [20, 21] 3. Acceptance and commitment therapy (ACT) [22, 23] |
| Procedure | Cole’s seven-step group dynamics that consisted of introduction, activity, sharing, processing, generalising, application, and summary. [ 19 ] |
| Duration | The resilience programme was conducted once a week for a period of 11 weeks for 60 minutes each time. [16, 17, 20] |
| Samples size | The participants were divided into the experimental and control groups. The experimental group was divided into five groups. Each group had 6-7 participants based on the appropriate number of group members. [ 19 ] |
| Activities |
This programme was adopted in an online version by a video conference through the Zoom application because of the COVID-19 pandemic.
1 st week “Resilience awareness”: The researchers and the participants engaged in activities to build relationships. The researchers taught about the resilience concepts and resilience components; such as, external support, self-awareness, abilities, and skills. 2 nd week “Situation awareness”: The researchers taught about thought and behavioural assessment. The researchers guided the participants to specify and analyse their academic problems according to the CBT. 3 rd week “My emotion”: The researchers guided the participants to observe their present emotions and other emotions. The researchers gave assignments to the participants. The emotional self-monitoring assignment was observing their emotions while facing academic problems. 4 th week “Emotional relaxation”: The researchers taught relaxation techniques to the participants; such as, muscle relaxation, cost-benefit analysis, and pie chart. After that, the participants applied the techniques to their academic problems. 5 th week “My identity”: The researchers guided the participants to observe their self-awareness; such as, strengths, weaknesses, self-esteem, and ideal self. 6 th week “How am I?”: The researchers guided the participants to observe their self-awareness from others’ perspectives and analyse their strengths to cope with their academic problems. 7 th week “Positive communication”: The researchers taught positive self-talk and positive talk techniques with others for the participants. The participants practiced communication skills through role-play activities. 8 th week - “I have”: The researchers guided the participants to analyse their academic problems, realise their external supportive factors, and apply their external supportive factors for coping with their academic problems. 9 th week “Brainstorm”: The researchers promoted the participants’ problem-solving skills through simulations of academic problems. 10 th week “My future”: The researchers guided participants to be aware of their future goals and prepare themselves for future situations. 11 th week “I’m ready”: The researchers reviewed the resilience concept by giving the participants analysis of what they had learned to apply to their academic problems. |
2.4. Statistical Analysis
The data were analysed by SPSS version 22. Descriptive statistical analysis was used for analysing the general information, resilience score, academic performance, and satisfaction. An independent t-test was used to identify the differences in the resilience score, academic performance, and satisfaction between both groups at the baseline and post-test. A paired t-test was used to analyse differences in the resilience score, academic performance, and satisfaction between the pretest and post-test in each group. All analyses used 95% confidence intervals, and the significance level was p-value < .05.
3. RESULTS
The results are shown in two phases: 1. The developing resilience programme phase and 2. evaluating the effect of the resilience programme phase.
3.1. The Developing Resilience Programme Phase
The resilience programme was verified for content validity using the IOC by five mental health specialists. This resilience programme had an IOC score of more than 0.50, which the IOC ranged between 0.60 to 1.0. The average IOC was 0.78. (Table 2).
3.2. Evaluating the Effect of the Resilience Programme Phase
The results in evaluating the effect of the resilience programme phase were divided into four parts: 1. General information, 2. the participants’ academic problems, 3. resilience, and 4. academic performance and satisfaction.
3.2.1. General Information
From Table 3, the control group and experimental group had no differences in the general information. In the control group, a total of 69.70% of the control group were female. The socio-economic status of their family had money remaining (66.70%), and the average monthly income per household was between 25,001 and 50,000 Thai Baht (48.50%). Their residential style was allocated villages, single houses, and townhouses (84.90%). The parents’ marital status was together (94.00%), and the control group had warm family relationships (60.60%). In academic performance, they had a grade point average between 3.50 and 4.00 (87.90%). In the experimental group, a total of 69.70% were female. The socio-economic status of their family had money remaining (48.50%), and the average monthly income per household was between 10,001-25,000 Thai Baht (33.30%). Their residential style was allocated villages, single houses, and townhouses (75.80%). The parents’ marital status was together (81.80%), and the experimental group had warm family relationships (72.70%). In academic performance, they had a grade point average between 3.50 and 4.00 (90.90%).
| No. | Items | IOC |
|---|---|---|
| 1 | Conformity to theory | 1.00 |
| 2 | Appropriateness of the programme’s name | 1.00 |
| 3 | Appropriate sorting of activities | 0.60 |
| 4 | Content suitability is consistent with the objectives | 0.60 |
| 5 | Appropriateness of the programme’s duration | 0.80 |
| 6 | Appropriateness of the equipment | 1.00 |
| 7 | Consistency between the assessment and objectives | 0.60 |
| 8 | Consistency between the activities and programmes | 0.60 |
| The average IOC | 0.78 | |
| General Information | Control Group | Experimental Group |
Asymp. Sig
(2-Sided) |
||
|---|---|---|---|---|---|
| n=33 | % | n=33 | % | ||
| Gender Male Female |
10 23 |
30.30 69.70 |
10 23 |
30.30 69.70 |
1.000 |
| Family’s socio-economic status Have money remaining. Have enough money. Have debt. |
22 11 0 |
66.70 33.30 0.00 |
16 15 2 |
48.50 45.50 6.00 |
.168 |
| Average monthly income per household (Thai Baht) < 10,000 10,001-25,000 25,001-50,000 50,001-100,000 more than 100,001 |
1 5 16 9 2 |
3.00 15.20 48.50 27.30 6.00 |
1 11 10 7 4 |
3.10 33.30 30.30 21.20 12.10 |
.337 |
| Residential style Allocated villages/single houses/townhouses Commercial building Condominium Slum Etc. |
28 1 0 3 1 |
84.90 3.00 0.00 9.10 3.00 |
25 4 1 1 2 |
75.80 12.10 3.00 3.00 6.10 |
.367 |
| Parents’ marital status Live together Separated Divorced Parents have died Father died Mother died |
31 1 1 0 0 0 |
94.00 3.00 3.00 0.00 0.00 0.00 |
27 2 2 0 1 1 |
81.80 6.10 6.10 0.00 3.00 3.00 |
.567 |
| Family relationship Warm relationship Sometimes quarrel Quarrel regularly |
20 12 1 |
60.60 36.40 3.00 |
24 7 2 |
72.70 21.20 6.10 |
.366 |
| Grade point average 3.50-4.00 3.00-3.49 2.50-2.99 < 2.49 |
29 4 0 0 |
87.90 12.10 0.00 0.00 |
30 2 1 0 |
90.90 6.10 3.00 0.00 |
.431 |
3.2.2. The Participants’ Academic Problems
The identification of the academic problems of the participants was received from the COPM. The participants determined the different academic problems, which were divided by intrinsic factors and extrinsic factors (Table 4).
3.2.3. Resilience
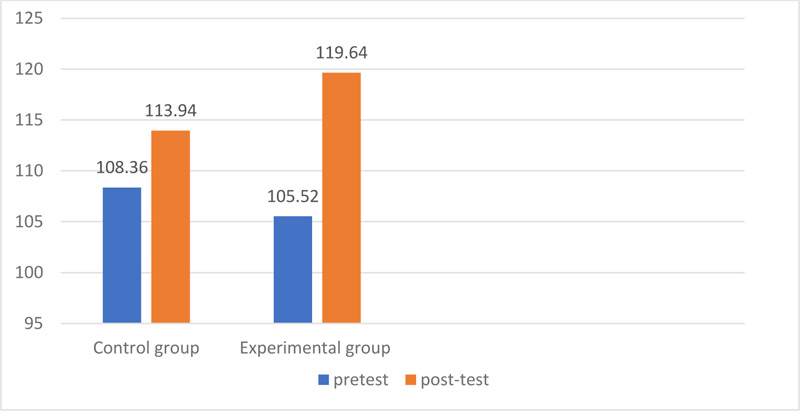
The resilience scores were used to compare the pretest and post-test of the participants in the control and experimental groups in the programme. The analysis of the comparative data on the pretest and post-test resilience scores showed a statistically significant difference in the effectiveness of the resilience programme through the group’s dynamics on changes in the resilience scores between the pretest and post-test in the control and experimental groups (p<0.05 and p<0.01) (Table 5; Fig. 2).
In terms of the data, the results of the comparison of the pretest and post-test resilience scores between both groups found that there was no statistically significant difference in the post-test resilience scores between both groups (Table 6).
Table 4.
| Academic Problems | |
|---|---|
| Intrinsic Factors | Extrinsic Factors |
| Students did not finish the assigned tasks on time. | Poor Internet connection. |
| Divisions on the study. | Electricity interruption. |
| Students felt bored while studying online. | The study environment was not conducive for studying; such as, devices, rooms, disturbances by the external environment, etc. |
| Did not understand the content of the lesson. | Students had workloads during online education. |
| Students felt stressed while studying online. | Online learning affected health. |
| Students had low motivation to participate in their studies. | Did not meet friends. |
| Studying online made learning more difficult to understand than studying at school. | Studying online made it difficult to understand the lesson. |
| Students felt anxiety. | The teacher taught quickly and did not explain the content clearly. |
| Time management. | Other academic problems. |
Table 5.
| The Participants | Pretest | Post-test | t | P-value |
|---|---|---|---|---|
| Mean ± S.D. | Mean ± S.D. | |||
| Control group (n=33) | 108.36 ± 17.394 | 113.94 ± 16.058 | -2.587 | .014* |
| Experimental group (n=33) | 105.52 ± 21.796 | 119.64 ± 17.412 | -3.938 | .000* |
| Test | Control Group (n=33) | Experimental Group (n=33) | t | P-value |
|---|---|---|---|---|
| Mean ± S.D. | Mean ± S.D. | |||
| Pretest | 108.36±17.394 | 105.52±21.796 | .587 | .559 |
| Post-test | 113.94±16.058 | 119.64±17.412 | -1.382 | .172 |
| Test |
Control Group (n=33)
Mean ± S.D. |
Experimental Group (n=33)
Mean ± S.D. |
t | P-value |
|---|---|---|---|---|
| The differences in the pretest and post-test resilience scores. | 5.576 ± 12.382 | 14.121 ± 20.600 | -2.042 | 0.045* |
When comparing the differences of the pretest and post-test resilience scores between the control and the experimental groups, it was found that there was statistically significant differences (p<0.05) (Table 7).
3.2.4. Academic Performance and Satisfaction
The comparison data of the academic performance and satisfaction between the pretest and post-test in both groups are shown in Table 8. There were no statistically significant differences between the control group's academic performance and satisfaction in the pretest and post-test. For the experimental group, there was a statistically significant difference in the pretest and post-test (p<0.01). Thus, it could be summarized that after treatment, the experimental group had an academic performance and satisfaction higher than before participating in this programme.
The comparison data of the academic performance and satisfaction between the control and experimental groups in the pretest and post-test are shown in (Table 9). In terms of academic performance, there was no significant difference in the pretest on academic problems between both groups. Moreover, in terms of academic satisfaction, there was no significant difference in the pretest on academic problems between both groups. However, in the post-test, there was a statistically significant difference in academic satisfaction between the control and experimental groups (p<0.01).
Table 8.
| The Participants | Academic Performance | t | P-value | Academic Satisfaction | t | P-value | ||
|---|---|---|---|---|---|---|---|---|
|
Pre-test Mean ± S.D. |
Post-test Mean ± S.D. |
Pre-test Mean ± S.D. |
Post-test Mean ± S.D. |
|||||
| Control group (n=33) |
6.11 ± 1.57 | 6.85 ± 1.98 | -1.868 | .071 | 5.87 ± 1.79 | 5.87 ± 2.29 | -.004 | .997 |
| Experimental group (n=33) |
6.03 ± 1.78 | 7.00 ± 1.38 | -3.216 | .003** | 6.25 ± 2.10 | 7.33 ± 1.80 | -3.878 | .000** |
| The Participants | Academic Performance | t | P-value | Academic Satisfaction | t | P-value | ||
|---|---|---|---|---|---|---|---|---|
|
Control Group (n=33) Mean ± S.D. |
Experimental Group (n=33) Mean ± S.D. |
Control Group (n=33) Mean ± S.D. |
Experimental Group (n=33) Mean ± S.D. |
|||||
| Pretest (n = 66) |
6.11 ± 1.57 | 6.03 ± 1.78 | .209 | .835 | 5.87 ± 1.79 | 6.25 ±2.10 | -.807 | .423 |
| Post-test (n = 66) |
6.85 ± 1.98 | 7.00 ± 1.38 | -.364 | .717 | 5.87 ± 2.29 | 7.33 ±1.80 | -2.877 | .005** |
4. DISCUSSION
The study of the effect of the resilience programme through group dynamics on the academic problems of Grade 7 students of Chiang Mai University Demonstration School can be discussed as follows:
The first item is resilience. After treatment, the control group and the experimental group had different changes in resilience because this programme was developed based on the CBT and ACT through the groups’ dynamics. As such, these therapies were effective in promoting resilience. The CBT was the process for assessing and understanding thoughts, affectiveness, body, and behaviour in several situations. Furthermore, the researchers used the ACT because this therapy focused on understanding, acceptance, and the present. Thus, it helped people to face adversity consciously. A combination of both therapies was also appropriate in promoting resilience. This programme was verified for the content validity using the IOC and validated the principles. The researchers practiced the procedures of the activities with other similar participants. Therefore, this programme was consistent with the theory, activities, procedures, duration, and early adolescent development.
Developing the resilience programme through the groups’ dynamics had a positive effect on resilience because the groups’ dynamics promoted individual learning and self- development through interaction with others in the group. People also learned new skills and had trust. In this research, the participants were early adolescents, who were concerned about social acceptance and friends. Therefore, developing the resilience programme through the groups’ dynamics was appropriate with the participants, as they could understand their academic problems, solve the problems, and learn from each other. Additionally, the participants reflected their learning in sharing, processing, generalising, and the application of the groups’ dynamics. In this research, the researchers gave an assignment, which helped the participants apply their skills, knowledge, and resilience components to cope with their daily academic problems. Moreover, the groups’ dynamics could be used to promote cohesiveness. Consequently, the participants coped with the academic problems together and learned to cope with the academic problem strategies from others. Comparing the current research with previous studies, it was found that previous studies had only focused on psychoeducation, whereas this research was a combination of psychoeducation and applying knowledge to cope with the academic problems. From the above, the experimental groups had a statistically significant difference in the pretest and post-test.
The findings could be discussed based on the psychological theories related to behaviour and early adolescent development as follows: In the post-test, the experimental group had increased resilience because they had learned under social conditions through the group’s dynamics. This was consistent with Erickson's psychosocial theory, which explained that adolescent psychosocial development was an effect of mental adaptation under social support [30]. The resilience components consisted of self-awareness. In the identity vs role confusion stage, early adolescents searched for their identity, so self-awareness could result in complete development. As such, they could perform according to their role. When discussing these findings based on Kohlberg’s moral development, it could be explained that the moral development stage in early adolescents was conventional morality. People performed by following their roles and social conditions [31]. From Piaget’s cognitive development theory, it could be explained that after treatment, the experimental group realised their abilities, themselves, and supportive factors that led to increased resilience, so they had formal operational cognition [32]. Developing this programme based on the CBT and ACT contributed to the participants analysing their academic problems. The process was consistent with the development, so the participants could learn appropriately. From previous studies, resilience was considered to be a dynamic process of positive adaptation. Therefore, it could be developed at any time. This would be because each person would have different resilience at varying times [7, 33, 34]. This supported the findings that the control group had different resilience scores between the pretest and post-test similar to the experimental group. However, Grotberg explained that resilience seemed easy to notice and promote, but in reality, not all children were resilient. This was due to the fact that their family did not contribute to the children’s resilience. Therefore, in the results of this present study, there were statistically significant differences in the resilience score in the pretest and post-test between the control and experimental groups. Hence, it could be summarised that this resilience programme could be used to promote individual resilience, and resilience should be promoted to early adolescents.
Secondly, the findings in the academic performance and satisfaction showed that this resilience programme emphasised promoting the resilience components. The experimental group practiced analysing their academic problems; as such, they could understand their automatic thoughts, emotions, behaviour, and body changes in-depth. The experimental group practiced a cost-benefit technique, pie chart, muscle relaxation, and diaphragm breathing. They realised themselves, and gained self-esteem from their perspective and others. About the skills and abilities, they learned positive communication skills, problem-solving skills, emotional assessment, and emotional management. Regarding the external supportive factors, they analysed their supportive factors, which helped them to cope with problems. As a consequence, they applied their resilience components to cope with their academic problems. Therefore, they had the strategies to cope with the problems, which led to increased academic satisfaction.
The findings in the academic performance and satisfaction were based on the Person-Environment-Occupation (PEO)model in the occupational therapy perspective. This programme focused on promoting the resilience components, which this was consistent with the PEO model. The resilience programme was used to contribute to the resilience components, self-awareness, skills, and a supportive environment. Self-awareness and skills were categorised in person according to the PEO model and recognised the supportive environment, which corresponded to the environment according to the PEO model. The increasing resilience and recognised supportive environment made it more consistent between the person and the environment. As a result, the students had increased academic performance and satisfaction, which was consistent with the PEO model. The PEO model was described as an occupational performance, as a result of the interaction between the person and the environment. If the environment corresponded with a person's interests and abilities, the person would increase their participation in the occupation and increase their ability to perform activities. If the person and environment were less consistent, then the person had less satisfaction in the occupational performance [35]. For the control group, there were no differences in academic performance and satisfaction between the pretest and post-test because they did not receive the programme. As a result, the control group did not have any positive adjustment to the academic problems. This made the composition of the person and environment less consistent. This caused the control group to have less participation in the activity, thus resulting in decreased academic performance and satisfaction.
From the results, it could be summarised that the resilience programme through the group’s dynamics could be applied to the contribution of resilience, academic performance, and satisfaction on academic problems.
LIMITATIONS AND RECOMMENDATIONS
This research study was conducted to collect data during the COVID-19 pandemic. As a consequence, this resulted in limitations in the group activities. Therefore, the researchers offered the following recommendations.
(1) This study used a quasi-experimental controlled study with a pretest and post-test. Long-term follow-up was not available, so future studies should include a follow-up on resilience, academic performance, and academic satisfaction.
(2) Future studies should apply and explore the effects of this programme in other age groups; such as, middle adolescents, late adolescents, or adulthood because each age group would have different important life activities.
(3) Future studies should also apply and explore the effects of this programme in different contexts.
CONCLUSION
This resilience programme, through group dynamics could contribute to the resilience, academic performance, and academic satisfaction with academic problems.
LIST OF ABBREVIATIONS
| COPM | = Canadian Occupational Performance Measure |
| CBT | = Cognitive-Behavioral Therapy |
| ACT | = Acceptance and Commitment Therapy |
AUTHORS' CONTRIBUTIONS
Chanakarn Kumkun worked on the entire study and coordinated the data analysis. Pornpen Sirisatayawong worked on data analysis. Supat Chupradit reviewed the literature, designed the research, collected and analyzed the data, and approved the manuscript.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Ethics Committee, Faculty of Associated Medical Sciences, Chiang Mai University, Thailand. Project number: AMSEC-64EX-018.
HUMAN AND ANIMAL RIGHTS
No animals were used for studies that are the basis of this research. All the humans used were in accordance with the Ethics Committee, Faculty of Associated Medical Sciences, Chiang Mai University, and the Helsinki Declaration of 1975.
CONSENT FOR PUBLICATION
Written informed consent was obtained from each participant prior to the study.
AVAILABILITY OF DATA AND MATERIALS
The data used to support the findings of this study are available on request from the corresponding author [S.C].
FUNDING
The study was financially supported by Graduate fund of Faculty of Associated Medical Sciences, Chiang Mai University, and Research Assistant by Young Researcher Fund, the Office of Research Administration, Chiang Mai University.
STANDARDS OF REPORTING
STROBE Guideline were followed.
CONFLICT OF INTEREST
This study had no potential conflicts of interest, financial, or otherwise, to declare.
ACKNOWLEDGEMENTS
The researchers appreciatively acknowledge the funding support from the Graduate School, Chiang Mai University, Thailand, and is grateful for all corresponding people in this study.

