All published articles of this journal are available on ScienceDirect.

The Impact of Complex Intervention on the Dynamics of Children’s Development with ASD
Authors Info & Affiliations
Abstract
Background:
The study of the complex development of a child with ASD is an important and relevant topic for discussion at the present moment. Complex intervention involves the interaction of specialists such as psychologists, speech therapists, speech pathologists, sensory integration and adaptive physical culture (APC) specialists for the rapid dynamics of children with ASD. To track the development of children, we used a comprehensive assessment of the child’s current skills – VB-MAPP.
Objective:
The objective of this study is to show the effectiveness of complex intervention in the correction of children with ASD.
Methods:
To track the development of children, we used a comprehensive assessment of the child's current skills – VB-MAPP. This test is the most widely used tool among behavioral analysts.
Results:
After processing the data, it becomes clear that the first group, which received classes from one specialist for 1 academic hour three times a week, has relatively low indicators of skill development compared to the second group. Children from the second group who received complex intervention from several specialists every day for 4 hours a day demonstrated positive dynamics in all areas of development.
Conclusion:
The results of the study confirm that the main condition ensuring the positive dynamics of the development of a child with ASD is the comprehensive intervention of specialists specializing in correctional work.
1. INTRODUCTION
Currently, autism spectrum disorder is one of the most discussed human conditions. According to the recent statistics, every 54th child in the world is diagnosed with autism spectrum disorder (ASD). Its increased prevalence brought it to the attention of society in the United States and worldwide [1]. Many scientists study autism as a disability or as a set of unique skills that they consider strengths [2], but at the sametime, the life path of people with ASD is very complex and challenging from early childhood to adulthood [3]. In addition, the main symptoms of autism spectrum disorder (ASD) include a lack of social communication and interaction [4].
In an effort to have a positive impact on this life trajectory, the staff of early intervention services, schools, clinics and other human service programs are looking for effective methods and techniques to work with children and youth with autism [5]. The elevated prevalence of autism [6] has also increased the demand for efficient educational and therapeutic services, and the science of interventions provides numerous data on methods that positively affect outcomes.
The purpose of our study is to identify the impact of a complex intervention on the dynamics of child development.
The major objectives of the project are the following:
1. To analyze theoretical approaches for solving the problem; the main theoretical approaches for studying the problem of childhood autism
2. To determine the appropriate sample for the study
3. To investigate the features of complex intervention delivered by professionals specializing in correctional work with autistic children
The diagnostic method of the research project includes experimental and empirical work that will be carried out at the center for the psychological and pedagogical correction of children with ASD in Nur-Sultan.
“Senim” (founded in 2012) was one of the first institutions in Kazakhstan to start helping children with autism spectrum disorder (ASD) and other developmental disabilities, as well as their families. During 10 years of this center’s operation, about tens of thousands of individuals with ASD and their relatives from different regions of Kazakhstan and neighboring countries received timely assistance and therapy.
The special rehabilitation program at the “Senim” center helped many kids to go to ordinary kindergartens and schools:
- Worldwide recognized diagnostic methods (VB-Mapp, etc.);
- Corrective and developmental methods with proven effectiveness (Evidence Based Practice): applied behavior analysis (ABA), DIR-Floortime, PECS and others;
- Methods of teaching speech and it’s development;
- Means of alternative and auxiliary communication;
- Sensory integration;
- Neuropsychological and psychomotor correction;
A comprehensive rehabilitation program for children with ASD is carried out in the following areas:
- Diagnosis of child’s condition;
- Early identification of children at risk;
- Correctional work with children older than 2 years and their preparation for kindergarten;
- Preparing for school and supporting children in the education system
The study involved 40 children with ASD aged 2 to 5 years. Of these, 29 are boys and 11 are girls. The sample was dominated by children of Kazakh ethnicity (80%). The condition of one child was complicated by epilepsy. Participants were selected based on the following criteria: presence of a diagnosis, age, absence of disorders of the perception systems (vision, hearing) and the musculoskeletal system, the presence of an understanding of reversed speech, the ability to follow instructions, the ability to imitate at the level of copying the actions of an adult in specially organized conditions. The study involved speaking and non-speaking children. The information necessary for the selection of participants was obtained during the parents' questionnaire.
2. LITERATURE REVIEW
2.1. Autism
Autism is a development disorder that is subject to neurobiological research. There are several reasons for this, and genetics plays a major role. According to the DSM-IV, the defining features of ASD involve violation of communication, speech, and socialization, as well as a narrow range of interests and activities. Mental retardation is common, but by no means ubiquitous. Children with ASD may possess superior cognitive abilities. Persistence, concreteness, poor emotional expression, and lack of understanding of other people's thinking can be striking. The neurological basis of many sensorimotor features of autism, including stereotypes, is unknown. It affects attention and sleep, and one-third of people with autism suffer from epilepsy in adulthood. Whether subclinical epilepsy plays a role in the regression of the development of one-third of toddlers, who lose their speech skills and become autistic, remains to be determined [7].
The theory of the “broken mirror”
There is also the theory of the “broken mirror”, which has attracted considerable attention far beyond the scientific community. This theory suggests that various socio-cognitive difficulties common in autism can be explained by the dysfunction of the mirror neuron system, which is believed to play a key role in imitation. The discovery of the mirror neuron system is one of the most important research achievements of neuroscience in the 20th century. Some scientists have reported that dysfunction of the mirror neuron system has been found in autism spectrum disorders (ASD). Finally, the theory of the “broken mirror” of RACES was announced in the mid-2000s. According to this theory, children with ASD cannot imitate the behavior of other people due to the dysfunction of the mirror neuron system; therefore, it is challenging for them to empathize with other people. However, the RAS does not always show problems with imitation. Researchers who criticized the theory of the “broken mirror” proposed a theory of “social modulation of the reaction from top to bottom.” According to this theory, the medial prefrontal cortex or temporoparietal junction, an area of the brain associated with mentalization, can modulate the system of mirror neurons in accordance with the social context [8]. All these features affect the social life of children and their close ones. Thus, in a study by Daulay et al. (2018), it was proved that mothers of children with autism spectrum disorders suffered parental stress to a greater extent compared with mothers raising children with other types of special needs [9].
The task of a specialist working in psychological and pedagogical correction centers is to assess the child's development, his/her needs and create a behavioral therapy program. The specialist should be able to make an individual correction program for each child and provide recommendations for parents on how to cope with learning difficulties of their own child. Specific work technologies should be close to the conditions in which the family and the child live and reflect their needs [10].
People with autism undergo various examinations throughout their lifetime to monitor their symptoms after rehabilitation treatment. For this reason, it would be useful to have a test that allows quick and accurate assessment of symptoms, as well as deepening critical areas. One of such diagnostic methods is the ADOS test. Pino et al. (2018) studied the practical application of FPA on ADOS-2 and showed its potential use for psychological evaluation of people with ASD and suggested further work to improve the quality of clinical evaluation [11].
Applied Behavioral Analysis (ABA)
There are many methods and techniques to teach and guide children with autism, only a few of them have become the subject of scientific research. The only method that has been confirmed by significant empirical studies is the method based on applied behavioral Analysis (ABA). The effectiveness of ABA has been confirmed by several hundred single-case experiments and a growing number of intergroup studies. Comprehensive ABA programs consist of several intervention procedures, such as discrete trial learning and natural environment learning, and are based on the basic principles of learning and motivation, such as positive reinforcement, quenching, stimulus control and generalization. The focus is on the observed behavior and how it is affected by environmental variables.
ABA (Applied Behavior Analysis) is an applied science that studies behavior based on the principles of behaviorism, where the basic concepts are behavioral reactions and unconditioned amplifiers. Dr. Ivar Lovaas, a behavioral psychologist, first applied ABA to autism at UCLA's Department of Psychology in 1987. He believed that social and behavioral skills could be taught even to children with deep autism using the ABA method. The idea was (and remains) that autism is a set of behavioral symptoms that can be changed or “extinguished”. When Lovaas first started using ABA, he did not hesitate to apply penalties for non-compliance, some of which could be very severe. This approach has been changed in most situations, but in some situations, it is still used. Whatever the opinion about Lovaas' approach (and many people believe that ABA is an unethical way of correcting behavior), his idea turned out to be absolutely correct: many, if not all, children, who underwent intensive ABA training, learned to behave in a socially acceptable way. The most basic method of Lovaas begins with the therapy of “discrete samples”. A discrete study consists of the therapist asking the child for a specific behavior (for example, “Jonathan, please take a spoon”). If the child follows the instructions, he is given “reinforcement” in the form of a treat, a five or any other reward that means something to the child. If the child does not follow the instruction, he does not receive a reward, and the instruction is repeated.
The specific content of the discrete sampling method is based on the assessment of a particular child, his needs and his abilities. Thus, a child who is already able to sort shapes will not be asked to sort shapes indefinitely for a reward, but he will focus on other, more complex social and/or behavioral tasks. The youngest children (under the age of 3) receive a modified form of ABA, which is much closer to play therapy than discrete trials. As they master behavioral models, specialists will begin to teach children in a natural environment, where they will be able to generalize the learned behaviors and include them in the usual social experience.
ABA can also be used in one of its many forms with older children, teenagers, or even adults. In addition, in order to conduct therapy individually or in a group, many therapists currently conduct ABA in natural settings, such as playgrounds, cafes and other public places. This approach makes it easier for children to immediately apply the acquired skills in a real situation [12].
Applied behavior analysis has proven that every child with developmental disabilities is able to learn; that, by operating with factors in the environment, it is possible to change a child's behavior, which means that by changing these factors, it is possible to help a person learn to live as comfortably as possible for him. At the same time, applied behavior analysis implies the continuous collection of data to assess the effectiveness of the intervention program. The main goal of the work of a behavioral specialist is to improve the quality of human life [13].
We assumed that the main condition that ensures the possibility of positive dynamics of the development of a child with ASD is a comprehensive intervention of specialists specializing in correctional work. The study of the complex development of a child with ASD is an important and relevant topic now.
Complex intervention involves the interaction of specialists such as psychologists, speech therapists, speech pathologists, sensory integration, and adaptive physical culture (AFC) specialists for the rapid dynamics of children with ASD.
3. MATERIALS AND METHODS
To track the development of children, we used a comprehensive assessment of the child's current skills – VB-MAPP. This test is the most widely used tool among behavioral analysts [14].
VB-MAPP was developed as a behavioral approach to assess language skills based on B.F. Skinner's analysis of verbal behavior. In his book “Verbal Behavior” (published in 1957), Skinner suggested that speech is learned behavior. VB-MAPP is an assessment based on the criteria of neurotypical speech development. It is applied for the students with developmental disabilities, who, as a rule, do not master speech in their natural environment.
VB-MAPP is an exhaustive tool that measures strengths and weaknesses in various stages of development, especially in the field of language and obstacles to the acquisition of skills. In addition, it provides an extensive checklist to track progress over time. Each part of VB-MAPP provides a team of behavioral specialists with important information that will be used in the development of a child behavior correction program. VB-MAPP testing is easily organized into three sections, which are all used to evaluate and track student progress. Students' skills are regularly reviewed in the main language and academic areas (listed below) at regular intervals to ensure the effectiveness of the program.
The first section of VB-MAPP is an assessment of the main stages. It measures sixteen skills on three levels:
1. Mand (request skill). The child says “cookies” when he wants cookies.
2. Tact (naming skill). The child points to the car and says “car”.
3. The behavior of the listener (the skill of understanding the reversed speech). The child hears “clap”, and then claps his hands.
4. Visual perception skills and pattern matching (matching visual stimuli). The child is given a picture and asked to find a match for it.
5. Game skill. A diverse and independent child's game.
6. Social skill. The child is able to interact with other people.
7. Imitation skill. A child can repeat various movements after an adult or a peer.
8. The skill of echo reactions (the child repeats what he heard). The child hears “mom” and repeats “mom”.
9. Spontaneous vocal behavior (babbling). The child makes vocal sounds without any prompting [15].
“Speech and Social Interaction Skills Assessment Program for Children with Autism and Other Developmental Disabilities” (VB-MAPP) was developed by Dr. Mark Sandberg (PhD, BCBA-D) in 2008. The results obtained during the testing of VB-MAPP became a reliable basis for the development of an effective training program with priority for the development of speech and social skills. This tool is based on typical child’s development and contains a detailed description of each of the three age stages: from 0 to 18 months, from 18 to 30 and from 30 to 48 [16].
For the study, we studied the VB-MAPP tests of 40 children with ASD aged 2 to 5 years attending the Senim Center, Nur-Sultan for 3 months. Out of 40 children, 2 groups were formed for comparison: 20 children in the first group received classes from one specialist for 1 academic hour 3 times per week and 20 children in the second group received complex intervention from several specialists daily for 4 hours per day. As a rule, these interventions were carried out with high intensity (at least 20 hours a week) that was ensured by the teamwork of specialists. All children had an individual learning plan.
The main skills that children learned and will be included for comparison: the skill of asking (MAN), understanding speech, TACT (name), imitation, the skill of visual perception, gaming and social skills.
Fig. (1) shows an example of the VB-MAPP test of a child from the first group
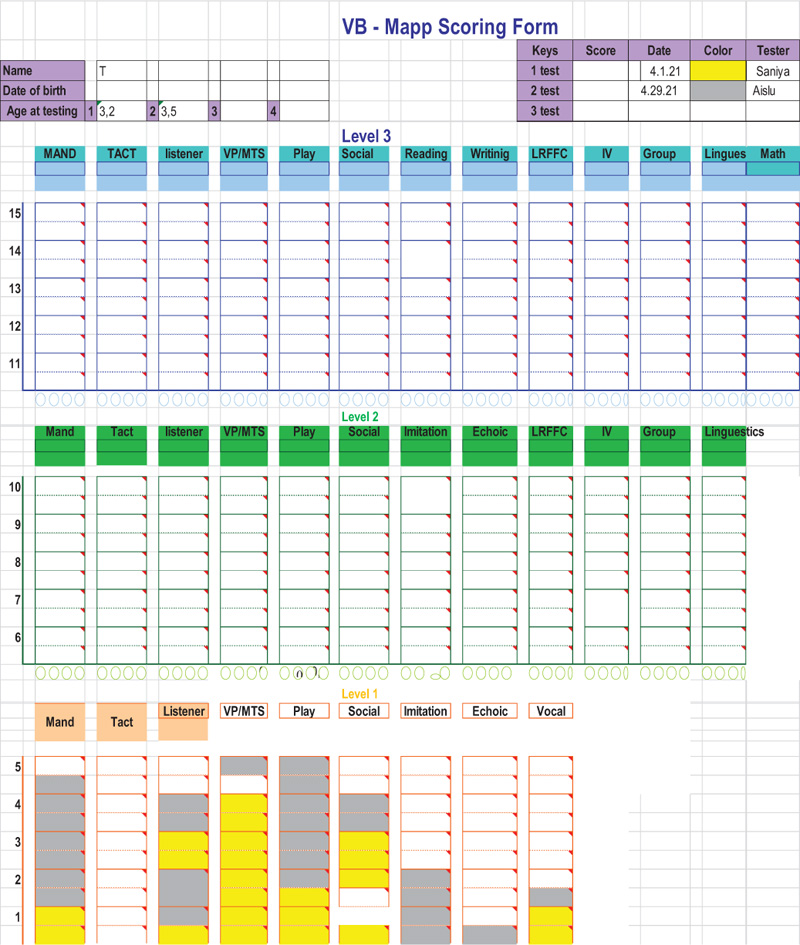
According to Fig. (1), child attended specialist classes 1 hour 3 times per week. Thanks to the assessment of VB-MAPP in the field of social skills and imitation, it was possible to identify gaps in the development of skills at the 1st level: he did not come into contact with a peer on his own initiative, did not offer an interesting subject to a peer and did not make a request, did not respond to the requests of other children, did not imitate their actions, and so on. There was also a complete lack of TACT (naming) skill.
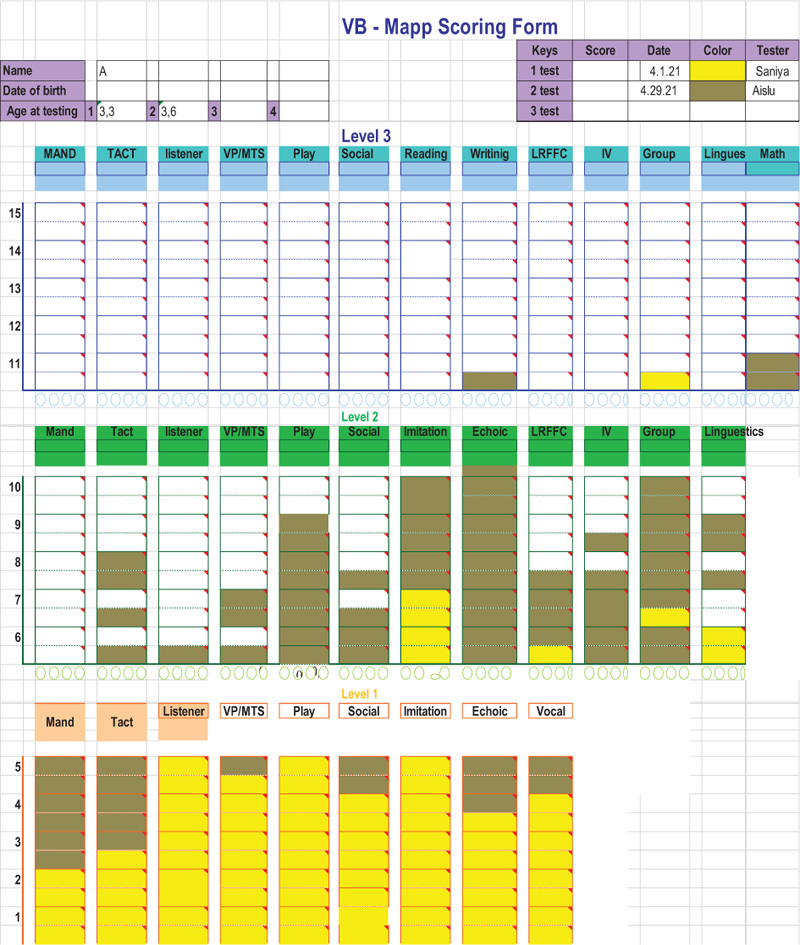
Fig. (2) shows an example of a test of a child from the second group, who visited the center every day for 4 hours per day for 3 months with all specialists.
According to Fig. (2), child used oral speech and built phrases of 1-2 words. The level of the game was combinatorial: child was able to build simple constructions. The child’s favorite game was playing with cars. Before the program, child experienced some difficulties. Thanks to the VB-MAPP assessment, a positive dynamic of the child’s development in all skills was revealed.
4. RESULTS AND DISCUSSION
The quantitative results of the first group, presented in Table 1, show that the level of skill development over 3 months of training did not give a positive dynamic.
The quantitative results of the second group, presented in Table 2, demonstrate the positive dynamics of children's development.
| No | Name | Mand | Tact | The Behavior of the Listener | Visual Perception Skill | Social Skill | Independent Play | Motor Imitation | Echoic | Spontaneous Vocal Behavior |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | A.T. | 4 | 0 | 4,5 | 4 | 3,5 | 4,5 | 2 | 1 | 1,5 |
| 2 | B.Y. | 2 | 0 | 2 | 4,5 | 2 | 4 | 3 | 1 | 0 |
| 3 | А.А | 3 | 0 | 3 | 2 | 1 | 4 | 2 | 1 | 1 |
| 4 | B.T. | 2,5 | 0 | 2,5 | 3,5 | 3,5 | 4 | 4,5 | 1 | 1 |
| 5 | A.D. | 1,5 | 0 | 2 | 1 | 3 | 4 | 2 | 0 | 1 |
| 6 | A.X. | 4 | 0 | 1 | 2,5 | 4 | 4,5 | 2 | 0 | 0 |
| 7 | A.N. | 4,5 | 1 | 4 | 4 | 0 | 2 | 3,5 | 3 | 1 |
| 8 | A.K. | 2,5 | 0 | 3 | 4 | 3,5 | 3 | 1 | 0 | 1 |
| 9 | G.K. | 3 | 0 | 3,5 | 4,5 | 2 | 0 | 4 | 0 | 0 |
| 10 | D.A. | 3,5 | 0 | 1,5 | 4 | 2 | 2,5 | 4,5 | 0 | 0 |
| 11 | I.A. | 4 | 2 | 2 | 4 | 1 | 4 | 3 | 3 | 1 |
| 12 | K.G. | 3,5 | 0 | 4,5 | 4 | 4,5 | 3,5 | 2 | 0 | 0 |
| 13 | K.A. | 1,5 | 3 | 1 | 3,5 | 0 | 4 | 3,5 | 3 | 1 |
| 14 | L.D. | 2,5 | 0 | 3,5 | 2,5 | 2,5 | 3 | 2 | 0 | 0 |
| 15 | M.S. | 2 | 1 | 2,5 | 3 | 3,5 | 4,5 | 3 | 3 | 2 |
| 16 | O.A. | 2 | 1 | 4 | 4 | 3 | 2,5 | 3,5 | 2 | 2 |
| 17 | P.D. | 4 | 0 | 4 | 4 | 2 | 1 | 2 | 0 | 0 |
| 18 | C.C. | 3 | 0 | 4,5 | 4,5 | 1 | 4,5 | 4 | 0 | 0 |
| 19 | T.Zh. | 4 | 2 | 3 | 4 | 2,5 | 2 | 4,5 | 3 | 2 |
| 20 | Sh.B. | 1 | 0 | 2 | 3,5 | 3 | 2 | 3 | 0 | 0 |
| Nº | Name | Mand | Tact | The Behavior of the Listener | Visual Perception Skill | Social Skill | Independent Play | Motor Imitation | Echoic | Spontaneous Vocal Behavior | Intraverbal | Group and Classroom Skills | Linguistic Structure |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | A.N. | 4,5 | 7 | 4,5 | 6 | 6,5 | 8,5 | 10 | 10 | 4,5 | 3 | 5,5 | 2,5 |
| 2 | A.D. | 5 | 6 | 8 | 7 | 5,5 | 10 | 10 | 10 | 7 | 2,5 | 3,5 | 3 |
| 3 | A.P. | 5 | 5,5 | 9 | 6,5 | 7 | 5,5 | 10 | 8,5 | 7 | 3 | 4,5 | 3 |
| 4 | B.S. | 5 | 7 | 10 | 7 | 6 | 6,5 | 10 | 6,5 | 8 | 3 | 3 | 3 |
| 5 | K.A. | 4,5 | 8 | 7 | 6 | 8 | 7 | 8 | 9 | 5,5 | 3 | 3,5 | 3 |
| 6 | Zh.D. | 5 | 4,5 | 4,5 | 10 | 4,5 | 8 | 8 | 7,5 | 7 | 3 | 2,5 | 2,5 |
| 7 | I.F. | 5 | 7 | 5 | 5 | 6,5 | 8 | 10 | 10 | 7 | 4 | 3 | 2 |
| 8 | K.A. | 4,5 | 7 | 6,5 | 8 | 7 | 8 | 8 | 10 | 6,5 | 3,5 | 4 | 2,5 |
| 9 | M.B. | 4 | 5 | 5 | 9 | 7 | 6,5 | 5,5 | 10 | 8 | 4,5 | 3 | 2,5 |
| 10 | M.D. | 4 | 5 | 7 | 10 | 8,5 | 9 | 10 | 10 | 8 | 3 | 4,5 | 2 |
| 11 | C.B. | 5 | 8 | 7 | 8 | 9 | 9 | 10 | 8,5 | 7,5 | 2,5 | 3 | 2 |
| 12 | C.E. | 5 | 7 | 8 | 7 | 4,5 | 7,5 | 10 | 7,5 | 9 | 3 | 2,5 | 3 |
| 13 | T.A. | 5 | 3 | 4,5 | 6,5 | 6,5 | 6,5 | 8,5 | 10 | 8,5 | 3 | 3 | 3,5 |
| 14 | C.A. | 5 | 4 | 6 | 4 | 7 | 7 | 10 | 10 | 10 | 3 | 3 | 2 |
| 15 | P.A. | 5 | 4,5 | 5 | 5,5 | 7 | 7 | 6,5 | 8,5 | 10 | 4,5 | 3 | 2,5 |
| 16 | K.N. | 4,5 | 5 | 5 | 6 | 6,5 | 8 | 10 | 6,5 | 7,5 | 3 | 4,5 | 3 |
| 17 | P.B. | 5 | 6 | 7 | 7 | 8 | 5,5 | 10 | 7,5 | 8 | 3 | 4,5 | 3 |
| 18 | D.B. | 4,5 | 6 | 6 | 8 | 10 | 6 | 8,5 | 10 | 8,5 | 1,5 | 3 | 2,5 |
| 19 | B.Zh. | 5 | 6,5 | 5,5 | 10 | 8,5 | 6 | 10 | 10 | 4,5 | 2 | 2,5 | 3 |
| 20 | A.N. | 5 | 5 | 4,5 | 6,5 | 9 | 7 | 8,5 | 10 | 8 | 3 | 2,5 | 2,5 |
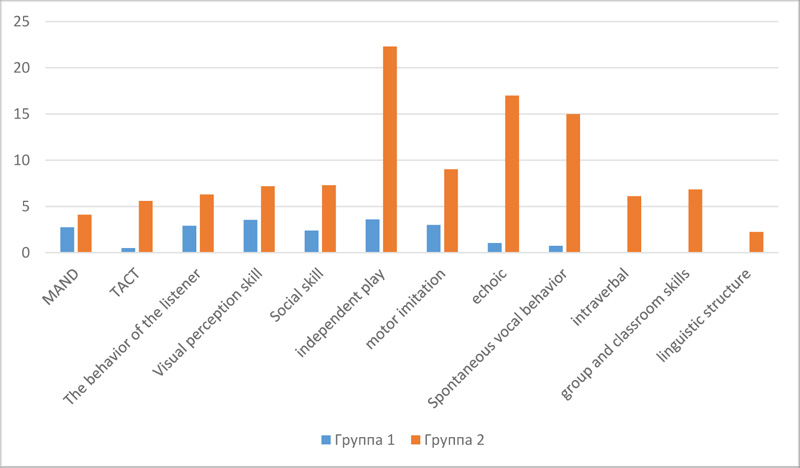
Fig. (3) shows the comparative results of the first and second groups.
After processing the data, it is clear that the first group has relatively low indicators of skill development compared to the second group. The children from the second group demonstrated positive dynamics in all areas of development.
CONCLUSION
The most important area of correctional work for children with ASD is assistance in the development of social interaction, adaptation skills, psychological and pedagogical correction. And here a natural shortage of professionals, who have the knowledge, skills and desire to work with children, is clearly revealed. Today Kazakhstan needs to create a system that guarantees lifelong support for children with autism spectrum disorders starting from its early detection. There is no complete cure for autism, so it is necessary to meet special needs of children in education and life and guarantee all kinds of necessary assistance for them.
Of course, the solution to the problem of early childhood autism can only be achieved by organizing serious and purposeful work of professionals, who are familiar with all details and are ready to learn new techniques. Therefore, it is important to train and develop a new generation of specialists, and create competent teams to help children and their families.
Today there is a certain number of private centers (mainly only in large cities of Kazakhstan) dealing with the problems of ASD-related correctional work. Attempts are being made at the State level to resolve issues related to childhood autism, but there are still no planned strategy and coordination in solving the problems of providing children with necessary ASD institutions and competent specialists. The study of the psychological characteristics of specialists working with children with ASD is the potential goal of future research.
In summary, the results of the study confirm that the main condition ensuring the positive dynamics of the development of a child with ASD is the comprehensive intervention of specialists specializing in correctional work. Professional interaction based on a common understanding of the characteristics of the child, the collective responsibility of team members for the results and consistency of actions comprise the most effective work plan.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
No human and animals are used for the basis of this research.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

