All published articles of this journal are available on ScienceDirect.

Impact of COVID-19 on Psychological Wellbeing of University Employees: The Mediating Role of Coping Mechanism
Abstract
Background:
The study aims to analyse the employees’ well-being in the COVID-19 pandemic scenario, by studying the mediating impact of coping behaviour in terms of stresses and negative experiences. The study scope is university teaching and staff personnel, constantly using online methods to deliver teaching-learning-evaluation processes.
Methods:
Empirical data was collected from 571 university employees through an online survey. The survey instruments were standard scales to assess the impact of events; distress, anxiety & stress, coping strategies, and personal well-being. The data was collected over a week after a month-long lockdown and analysed through CFA and SEM tools.
Results:
The role of coping strategies remains central to pandemic or emergency conditions. Statistical analysis shows that distress, anxiety and stress have adversely impacted the coping strategies and well-being of the respondents. The members were identified based on their responses and suitable measures being instituted to strengthen their coping strategies and abilities to deal with adverse situations.
Conclusion:
This study contributes to the literature by presenting and validating a theory-driven setting that highlights the degree of negative consequences of the Covid-19 pandemic and lock-down conditions. This research establishes the usefulness of tested personal wellness theories in a non-clinical setting.
1. INTRODUCTION
The calamitous effects of global pandemics are not unfamiliar to human history. The 1918 Influenza pandemic, infamously known as the “Spanish Flu,” engulfed the world in three distinct waves over a span of more than three years, infecting nearly half of the global population and resulting in over 50 million fatalities. Fast forward to the 21st century, the world has been confronted with another pandemic of comparable scope-COVID-19. First emerging in late 2019, this highly infectious disease has brought even the most advanced healthcare systems to their knees, manifesting in a series of devastating waves in 2020 and 2021.
India, a country with an intricate public health infrastructure, initially appeared to take successful preventative measures against the first wave of the COVID-19 pandemic. A nationwide lockdown was initiated in March 2020, which led to a temporary slowdown in case numbers, providing a momentary sense of victory [1]. Public health experts and epidemiologists noted that this lockdown helped bolster healthcare facilities by providing a window for ramping up testing capabilities and other medical resources [2]. However, the complacency that followed proved costly when the second wave struck with unparalleled fury in April 2021. This wave was primarily driven by a new and more virulent strain of the virus, known as the B.1.617 or Delta variant [3]. Despite the Indian government's establishment of a SARS-CoV-2 Genomic Consortium for genomic sequencing, the emergence of this new variant caught healthcare systems, policymakers, and researchers off-guard [4]. The second wave led to unprecedented pressure on India's healthcare system. There were catastrophic shortages in essential medical supplies, including ventilator beds, oxygen, and critical medications such as Remdesivir. Epidemiological studies and health system reviews pointed to systemic failures and resource mismanagement as contributing factors to this collapse [5]. Amidst the already complicated landscape, a series of new health challenges emerged. The rise of Mucormycosis, commonly known as Black Fungus, was a disturbing phenomenon observed in post-COVID patients [6]. Scientific studies have indicated that this could be linked to prolonged hospital stays, excessive use of steroids, and immunocompromised states, complicating the already intricate treatment protocols [7]. The societal ramifications were equally dire. Public panic was exacerbated by media portrayals and real-life experiences such as the sight of floating bodies in rivers and the looting of medical supplies. Social studies have documented how misinformation and lack of reliable communication led to heightened public anxiety [8]. One distinguishing feature of the second wave in India was its impact on younger populations, contradicting earlier beliefs that they were at a lower risk. Studies indicate that this might have been due to multiple factors, including lax behavior during the period between the two waves and variations in vaccination coverage among different age groups [9]. By carefully examining India's unique scenario, this study aims to contribute nuanced perspectives to the global understanding of the COVID-19 pandemic and its varied impacts on different populations and infrastructures.
The pandemic's progression, notably captured by social and visual media, contributed significantly to widespread anxiety and panic. Unsettling images of overflowing hospitals, people gasping for oxygen, bodies floating in rivers, and numerous other grim realities bombarded the collective conscience of the nation. The media also discussed the continuously mutating strains, adding another layer of uncertainty and anxiety to an already distraught populace [5].
The pandemic's onset has led to a paradigm shift in academic institutions worldwide, one that has not only affected the modus operandi but also trickled down to the psychological well-being of university employees [1]. The shift to virtual learning environments, remote administrative work, and abrupt changes to academic protocols have presented unprecedented challenges for faculty, administrative staff, and support services alike [2]. The abrupt transition to online teaching has been stressful for faculty members, not just from a technical standpoint but also pedagogically. The loss of face-to-face interactions and the absence of immediate feedback have led to an emotional void, making educators question their teaching efficacy [3]. Such situations have resulted in heightened stress levels and even instances of burnout [4]. Work-from-home conditions, initially considered a boon by many, soon morphed into a bane as the lines between professional and personal life blurred. Academic employees found themselves caught in a 'role-conflict,' trying to balance professional responsibilities with household chores, and child or elder care, leading to increased levels of anxiety and depression [5]. University administrative staff faced their own set of challenges. In addition to adapting to remote working conditions, they were tasked with implementing unprecedented emergency measures, often with limited guidance. This resulted in increased workloads and diminished time for self-care, thereby affecting their overall psychological well-being [6]. Research has also indicated that the pandemic has exacerbated existing social inequalities among university employees. Those with limited access to technology, those caring for dependents, or those already suffering from mental health conditions found the new working conditions particularly challenging, contributing to a decline in overall well-being [7]. Initial studies have suggested that coping mechanisms such as social support, mindfulness exercises, and timely institutional interventions can alleviate some of the psychological distress experienced by academic employees [8]. However, the efficacy of these coping mechanisms varies greatly among individuals and warrants deeper investigation, a gap this study aims to address.
By diving deep into these multifaceted challenges, this research aims to develop a nuanced understanding of the impact of the COVID-19 pandemic on the psychological well-being of university employees. This will not only contribute to the existing body of knowledge but also provide actionable insights for policymakers and institutional leaders.
The present study aims to fill a critical gap in the existing literature by focusing on the psychological well-being of university employees in the context of the COVID-19 pandemic. Further, this research intends to shed light on the mediated role of coping mechanisms in mitigating the negative impacts of COVID-19 on psychological well-being. While there exists a considerable body of literature that explores the psychological well-being of healthcare workers, frontline staff, and the general population amid the COVID-19 pandemic, fewer studies have focused specifically on university employees. This study addresses this gap by examining the psychological impact of the COVID-19 pandemic on this overlooked demographic, particularly in the Indian context.
Most existing studies that discuss the psychological well-being of individuals during the pandemic tend to focus on diagnostic assessments or prevalence rates of psychological conditions. Our study adds a unique perspective by investigating how coping mechanisms mediate the relationship between COVID-19-related stressors and psychological well-being among university employees. This research contributes to the existing literature by focusing on India-a country that faced unique challenges during the pandemic, including a damaging second wave dominated by the Delta variant. Cultural norms and societal structures in India can substantially influence coping strategies and mental health outcomes, making this study valuable for understanding the unique coping mechanisms that university employees in India employ.
2. REVIEW OF LITERATURE
Traditionally, pandemics have been understood as events that lead to widespread illness and mortality, with their psychological impact being somewhat underrepresented in academic literature. However, the COVID-19 pandemic has brought mental health to the forefront, challenging traditional narratives that typically do not associate pandemics with psychological disturbances akin to post-traumatic stress disorders (PTSD) [5]. An earlier review by Brooks et al. in “The Psychological Impact of Quarantine and How to Reduce It” indicated that quarantine measures during epidemics like SARS, H1N1, and Ebola resulted in various psychological effects, such as confusion and anger [9]. Likewise, Pfefferbaum and North in “Mental Health and the COVID-19 Pandemic” argued that psychological outcomes could be a 'second wave' of the pandemic crisis [10]. These insights have broad implications for understanding the psychological toll of pandemics beyond merely counting cases or mortalities [11]. study published in the Journal of the American Academy of Child & Adolescent Psychiatry highlighted that the impact extends to children and adolescents, leading to increased instances of anxiety and depressive disorders. They found that social isolation measures exacerbated existing mental health problems among young people. Hawryluck et al. also demonstrated that participants who had been quarantined during the SARS outbreak experienced PTSD symptoms and depression for up to three years post-quarantine (Emerging Infectious Diseases, 2004). This long-term impact resonates with the growing concerns surrounding the lasting psychological effects of the Covid-19 pandemic. Hence, the cumulative evidence suggests that pandemics, traditionally viewed as medical and logistical crises, have profound long-term impacts on mental health, affecting both clinical outcomes and well-being across demographic groups. The COVID-19 pandemic has only reinforced the necessity of integrating mental health into pandemic preparedness and response strategies.
The pandemic has not only had broad societal impacts but has also exerted differential pressure on various demographics. A study [6] focused on the medical staff and the general public in Wuhan, China, where the pandemic originated. Utilizing the Impact of Event Scale-Revised (IES-R) and the Depression, Anxiety and Stress Scale (DASS-21), the study found that medical staff were more affected psychologically than the general public. About 51% of the respondents considered psychological counseling beneficial, with 66% of those being medical staff and 34% from the general public. Wang et al. [7] extended this research to a more international context, including seven middle-income Asian countries. The highest stress levels were observed in Thailand, while Vietnamese citizens reported the least. The study emphasized the need for early-stage psychological support for the general population. Another study [12] assessed the impact of lockdown measures on the general population in Reunion Island. The results revealed significant reductions in overall well-being and increased sleep disruption, anxiety, and sedentary behavior.
The shift to online learning due to the pandemic has had profound implications for the psychological well-being of both students and faculty. A study [13] elucidated that while hedonic motivation and facilitating leadership influenced the adoption of online teaching, it left questions about its impact on well-being. A study specifically focused on teachers in Spain and found increased levels of stress, anxiety, and depression [14]. Similarly, a study [15] noted that 73% of Italian university students surveyed were graded as depressed, and 35% as anxious, highlighting the emotional toll the pandemic took on students. This research aligns with findings from Son et al., who published a paper in “PLOS ONE” in 2020, demonstrating an uptick in anxiety and depressive symptoms among university students due to the pandemic. Educational settings are not just physical spaces for learning; they are also essential for socialization, emotional development, and mental well-being. As noted, the absence of a comprehensive mental health strategy in G20 educational systems during the pandemic was a significant oversight [16]. The transformation in educational settings, spurred by the pandemic, necessitates a deeper examination of its psychological impact on everyone involved, from students to faculty to administrative staff. Thus, the COVID-19 pandemic underscores the need to consider the psychological well-being of all stakeholders in educational settings, not just during the pandemic but as a fundamental aspect of educational policy and practice.
The COVID-19 pandemic has led to a major upheaval in higher education systems worldwide, with significant implications for the mental health and well-being of students, faculty, and staff. One of the critical studies in this context was conducted [16], which revealed that students' mental health and well-being were largely overlooked during the pandemic across the G20 countries. Research conducted [17] in the “Journal of Psychiatric Research” reveals that the abrupt shift to online learning, social isolation, and uncertainties related to academic progression has resulted in increased stress and anxiety levels among university students. Another study by Huckins et al., published in “JAMA Pediatrics,” demonstrated that college students showed a significant decrease in physical activity and an increase in screen time, which negatively affected their psychological well-being. Faculty members are also impacted. A study [18] in “Frontiers in Psychiatry” revealed that university staff experienced increased stress and burnout levels due to changes in teaching modalities and additional administrative work.
The global higher education landscape has thus become a critical area for assessing and addressing the multifaceted impacts on psychological well-being. It is evident from the existing literature that both students and educators are facing unparalleled mental health challenges. These findings necessitate urgent interventions and policies at the institutional and national levels to mitigate the negative psychological outcomes of this unprecedented crisis in global higher education. The research in this area underscores the importance of immediate, evidence-based interventions to improve mental health and well-being across higher educational institutions worldwide.
3. CONCEPTUAL MODEL
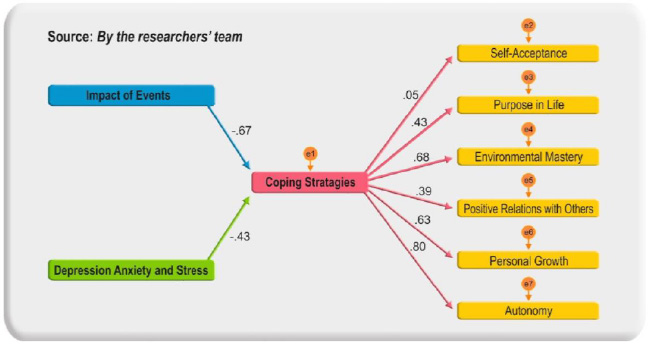
The interactive model looked at the ‘Impact of Event Scale’ and ‘Depression, Anxiety, and Stress Scale’ for effect-related inputs, which were assumed to be negative due to the prevailing pandemic and related events, based on employees’ personal experiences. ‘Coping Strategies Scale’ was used to
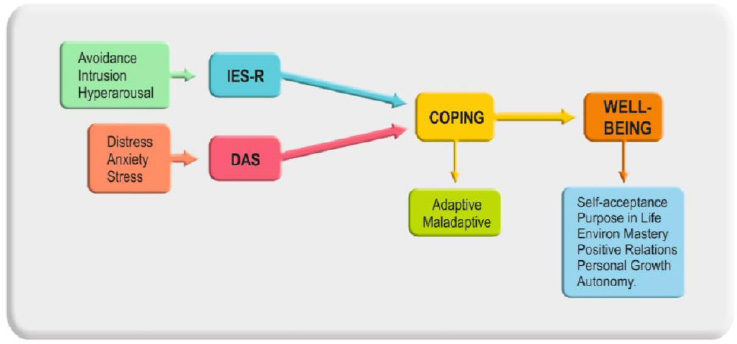
measure individual responses to facing personal difficulties, which as per the selected scale could make an employee either adapt to counter unwanted events or give in and become a victim of the same. This cumulatively leads to one’s well-being in the existing scenario, which was captured by utilising well well-established ‘Psychological Well-Being Scale’. The data for all these four constructs was captured through standard instruments. A conceptual model was evolved through iteration as given in Fig. (1).
4. METHODOLOGY
4.1. Study Design and Participants
The primary method of the research study was a cross-sectional survey. This coincided with nearly a month-long lockdown and work from home during April and May 2021. The survey was conducted from 17 to 21 May 2021. A standard questionnaire was cascaded to all the employees through their registered institutional e-mails through a Google form.
4.2. Sampling Design
Management had decided to conduct this ‘personal well-being’ survey of the entire population of the two campuses and corporate office; hence it was more or less a census study. The inclusion criteria were only the employees of Chitkara Universities, India with email IDs of Chitkara or Chitkara University.
4.3. Survey Instruments
A scan of the literature was carried out to assess similar studies across the globe during 2020 or 2021. This also provided available instruments for the current study since these survey instruments had been widely used and had higher reliability. Some of the references to such studies are given at the end of this paper. For this study, the following survey questionnaire was used:
4.3.1. The Impact of Event Scale-revised (IES-R)
The scale was developed to measure current subjective distress related to a specific life event [18]. Eventually, it was modified from 15 to 22 items [19], to measure intrusive, avoidance and hyper-arousal symptoms after such events. The IES has been used widely to investigate trauma-related distress like pandemic survivals, traffic accidents, war veterans, natural disasters, survivors of intensive care admission, cancer diagnosis, or any severe incident [18, 20].
4.3.2. Depression, Anxiety and Stress Scale (DASS-21)
Another personal outcome of traumatic events around us, DASS has 21 items in a set of three self-report scales, designed to measure emotional states. The scale is divided into three sub-constructs of depression, anxiety and stress with seven items each [21]. The DASS-21 in a clinical setting allows an observer to identify the locus of emotional disturbances, as a part of clinical assessment.
4.3.3. Coping Strategies Scale
The coping strategies questionnaire was developed by Rosenstiel and Keefe [22] using a pool of items reflecting strategies frequently reported by patients or survivors and deemed to be important by researchers and clinicians involved in the management of trauma. This 28-item questionnaire measures the use of strategies for coping with adverse events. The scale captures coping strategies at the individual level in the face of the existing situation of the pandemic. The scale divides items into adaptive (16) or maladaptive (12) states of individual responses [23].
4.3.4. Personal Well Being Scale
The fourth survey questionnaire captured the psychological well-being of each employee in the prevailing situation. Developed by psychologist Carol D. Ryff, the 18 or 42-item Psychological Wellbeing (PWB) Scale measures six aspects of well-being and happiness: autonomy, environmental mastery, personal growth, positive relations with others, purpose in life, and self-acceptance [24]. The scale used for the survey was based on 18- items, drawn from SPWB-18 (https://sparqtools.org/mobility-measure/psychological-wellbeing-scale/).
4.3.5. Legal Safeguards
The study design and protocols were approved by the Internal Ethics Committee of Chitkara University, India. Respondents were given an undertaking in the questionnaire that personal information would be fully safeguarded. Consent to participate in this study was indicated by respondents proceeding to the first page of the survey, which was emphasised in the opening remarks of the survey questionnaire itself. In case any specific personal reference is to be used, permission will again be obtained from the concerned respondent.
4.4. Demographic Profile – Faculty and Staff
4.4.1. Selection Criteria
This study utilized a stratified sampling technique based on biographical data, focusing on experience and gender as the primary criteria for inclusion. Experience is operationally defined to include both designation and age. Notably, the second wave of the pandemic disproportionately affected younger individuals, prompting the classification of employees with less than 10 years of experience as a separate cohort for analysis. In addition to the targeted clusters, a comprehensive analysis comprising all university employees was conducted, employing four main constructs.
4.4.2. Response Rate
The survey was distributed across three campuses of a large university in the North of India: Punjab (n=850), Himachal (n=130), and Corporate Office (n=100), totalling 1,080 faculty and staff. A total of 571 responses were collected by the cutoff date, yielding a response rate of approximately 53%.
4.5. Descriptive Analysis
Reference Table 1 for a brief overview of the data.
The survey of 571 faculty and staff shows a fairly balanced gender distribution with 265 females and 306 males. A majority (55%) have less than 10 years of experience. Notably, 17% reported having contracted COVID-19, and around 30% have cared for a COVID-affected family member. Regarding vaccinations, 53% have received at least one dose, and 21.7% have completed both doses. Most respondents reside with their full family (71.6%), and a sizable proportion hold a master's degree or higher (89.2%).
| Item | Sub-group | Number | Item | Sub-group | Number |
|---|---|---|---|---|---|
| Gender | Female | 265 | HighestQualification | Doctorate | 228 |
| Male | 306 | Master’s degree | 283 | ||
| Age (Years) | Over 60 | 11 | Degree/PG Diploma | 47 | |
| >40 to 60 | 158 | Diploma/Plus Two | 13 | ||
| >30 to 40 | 312 | Staying in current residence with | Parents | 81 | |
| <30 | 90 | Spouse | 46 | ||
| Experience (Years) | Over 20 | 32 | Children | 8 | |
| >15 to 20 | 69 | Full Family | 409 | ||
| >10 to 15 | 151 | Alone/in PG | 27 | ||
| <10 | 319 | - | - | - | |
| Had Covid 19 | 98 (Yes) | 473 (No) | Looked after a Covid patient | 174 (Yes) | 397(No) |
| Tested for Covid | 192 (Yes) | 379 (No) | Taken the first vaccination | 303 (Yes) | 250 (No) |
| Someone in the family had Covid | 130 (Yes) | 441 (No) | 18 (Not planning to take) | ||
| - | - | - | Taken both Vac | 124 (Yes); others not applicable | |
| S.No | Parameters | Female (265) | Male (306) | ||
|---|---|---|---|---|---|
| Numbers | Percentage | Numbers | Percentage | ||
| 1 | Personally, suffered from Covid-19 | 46 | 17% | 52 | 17.3% |
| 2 | Looked after self/family member suffering from Covid-19 | 89 | 33.6% | 85 | 27.8% |
| 3 | Tested for Covid-19 | 90 | 33.6% | 102 | 33.7% |
| 4 | Taken one Covid vaccination | 138 | 51.3% | 165 | 54.6% |
| 5 | Taken both shots of vaccination | 52 | 19.6% | 72 | 23.5% |
| 6 | Not planning to take yet | 9 | 3.4% | 9 | 2.9% |
| 7 | Extreme reactions (count 4 & 5) - IES | 833 | 3.14% | 766 | 2.5% |
| 8 | Extreme reactions (count 4 & 5) – DASS | 329 | 1.24% | 176 | 0.5% |
| 9 | Failing to cope with the situation (count 4 & 5) | 1664 | 6.27% | 2592 | 8.47% |
| 10 | Personal well-being appeared to be compromised (count 1 & 2) | 1236 | 4.66% | 1540 | 5.03% |
| S.No | Parameters | <10 years of Experience (319) | >10 years of Experience (252) | ||
|---|---|---|---|---|---|
| Numbers | Percentage | Numbers | Percentage | ||
| 1 | Personally, suffered from Covid-19 | 50 | 15.7% | 48 | 19.04% |
| 2 | Looked after self/family member suffering from Covid-19 | 83 | 26.01% | 91 | 36.1% |
| 3 | Tested for Covid-19 | 92 | 28.8% | 100 | 39.7% |
| 4 | Taken one Covid vaccination | 145 | 45.5% | 158 | 62.7% |
| 5 | Taken both shots of vaccination | 47 | 14.7% | 77 | 30.5% |
| 6 | Not planning to take yet | 16 | 5% | 2 | 0.08% |
| 7 | Extreme reactions (count 4 & 5) - IES | 873 | 2.70% | 290 | 1.15% |
| 8 | Extreme reactions (count 4 & 5) – DASS | 220 | 0.69% | 104 | 0.41% |
| 9 | Failing to cope with the situation (count 4 & 5) | 2572 | 8.06% | 726 | 2.88% |
| 10 | Personal well-being appeared to be compromised (count 1 & 2) | 1467 | 4.59% | 773 | 3.06% |
| Instruments | Qs (k) | Sum of Vars(∑Vi) | Vars of Sum ofEach Response (Vt) | Cronbach Alpha |
|---|---|---|---|---|
| Part B: Impact of Events | 22 | 25.83035262 | 214.5515503 | 0.921493791 |
| Part C: Depression Anxiety & Stress | 21 | 11.54089823 | 108.2891784 | 0.938096453 |
| Part D: Coping Strategies | 28 | 37.71914575 | 254.3093108 | 0.883223749 |
| Part E: Psychological Well-Being | 18 | 16.78123304 | 58.72246129 | 0.756241451 |
The table presents a gender-based analysis of the impact of COVID-19 on faculty and staff. It reveals marginal differences between males and females in contraction rates (17% vs. 17.3%) and testing (33.6% vs. 33.7%). However, males are slightly more vaccinated than females. Women exhibit more “extreme reactions” according to the IES and DASS scales. Additionally, men report higher rates of struggling to cope with the situation (8.47% vs. 6.27%) but also show a slight edge in compromised personal well-being (Table 3).
The table reveals a comparison of COVID-19's impact on faculty and staff based on experience levels. Staff with over 10 years of experience report higher rates of COVID-19 contraction, caregiving, and vaccination uptake compared to their less experienced counterparts. However, those with less than 10 years of experience show a higher propensity for extreme emotional reactions (as per IES and DASS) and greater difficulties in coping with the pandemic. Vaccine skepticism is also higher among the less experienced cohort.
5. DATA ANALYSIS
The data were subjected to validation testing to check their internal coherence and reliability. All constructs were found to be above the threshold value of 0.70 on Cronbach Alpha, as given in Table 4.
5.1. Impact of Events
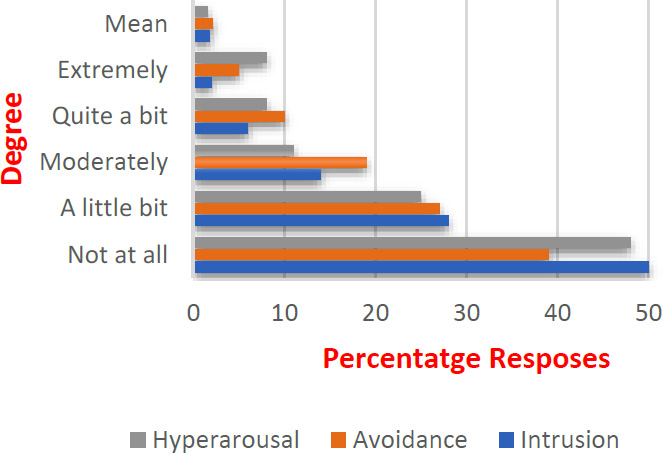
The survey on IES is divided into three responses. Intrusion or internalizing of adverse impact, avoidance of the same, or increased excitement as hyperarousal causing extreme stress. The responses show that over 46% of employees have remained unaffected in all three adverse reactions, while 27% were affected a little bit. Only 5% were affected severely (Table 5 and Fig. 2).
| Construct | Sub-Construct | Not At All | A Little Bit | Moderately | Quite a Bit | Extremely | Mean |
|---|---|---|---|---|---|---|---|
| Impact of Events (Percentage) | Intrusion | 50 | 28 | 14 | 6 | 2 | 1.82 |
| Avoidance | 39 | 27 | 19 | 10 | 5 | 2.14 | |
| Hyperarousal | 48 | 25 | 11 | 8 | 8 | 1.52 |
5.1.1. Intrusion
The Covid scenes, traumatic thoughts and consequent impact were extreme for a little over 2% of the respondents, while 6% and 14% were affected quite a bit and moderately respectively. The responses show that 50% did not show any effects, while 28% were affected a little bit. The average mean is 1.82, which shows positive responses to a reasonable extent.
5.1.2. Avoidance
The items of this sub-construct measured an individual avoiding the reality of virus-related panic or impact. About 5% of respondents attempted avoidance with 10% avoiding it quite a bit. Moreover, 39% did not require to avoid the effects while 27% had to make a little effort. The average mean of all items is 2.14, which reflects leaning towards a little bit and moderate avoidance of the situation.
5.1.3. Hyperarousal
The sub-construct looked at COVID events/news triggered by irritable nature, lack of sleep, or feeling of lack of concentration. Moreover, 48% of respondents did not encounter any of these adverse symptoms, while 25% felt a little bit. Almost 8% of respondents suffered extremely or quite a bit from these symptoms. Another 11% were moderately affected. Two hundred and four responded as attempting to be more watchful and cautious against COVID-19 symptoms.
5.2. Depression, Anxiety, and Stress
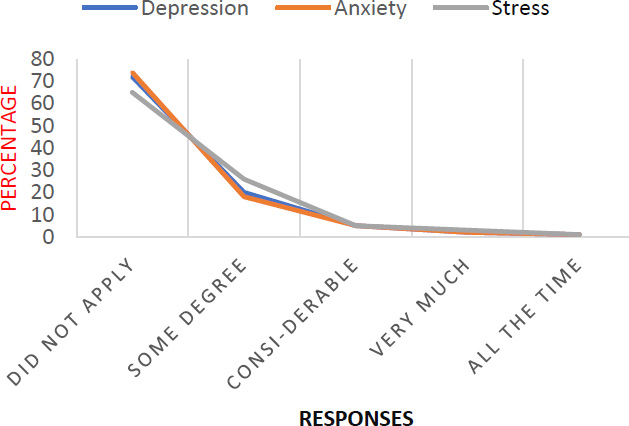
The survey questionnaire on this dimension provided data under three sub-constructs - depression, anxiety and stress. The results of this survey are very encouraging on this scale as just 1 to 3% of the respondents appear to be suffering from COVID-19 triggered adverse emotions, while above 70% responded as not affected at all. This is also evident from the average means of all items, which is closer to 1.40, implying that the effects of these dimensions were either not there or were only to some degree on most of the employees (Table 6 and Fig. 3).
| Construct | Sub-construct | Did Not Apply | Some Degree | Considerable | Very Much | All the Time | Mean |
|---|---|---|---|---|---|---|---|
| Depression, Anxiety, and Stress (Percentage) | Depression | 72 | 20 | 5 | 2 | 1 | 1.40 |
| Anxiety | 74 | 18 | 5 | 2 | 1 | 1.35 | |
| Stress | 65 | 26 | 5 | 3 | 1 | 1.47 |
5.2.1. Depression
The items in the sub-construct portray a lack of initiative, lower work-related enthusiasm, sinking feelings and hopelessness. Only 1 to 2% of the respondents felt overwhelmed, while 5% responded with considerable effects of these emotions. About 72% of the employees did not relate to any of such negative feelings, while 20% had some degree of depressive feeling. A mean average of 1.40 validates the results to be more positively inclined.
5.2.2. Anxiety
The items portray breathing difficulties, trembling, being scared or in panic. The responses were nearly identical to depression, as only 1 to 2% of the respondents felt overwhelmed with these emotions, while 74% didn’t feel any anxiety and18% were affected to some degree. The average of items means is 1.35, which projects positive responses.
5.3. Stress
Nervousness, difficulty in relaxing, agitation and sensitivity were some of the statements under this sub-construct. The responses were again identical to depression, as 65% didn’t feel any stress, while 26% felt stress to some degree. Only 1 to 3% of the respondents felt overwhelmed with these emotions.
5.3.1. Coping Strategies
The strategies reflect how the employees face adverse impacts, depression, anxiety, or stress due to prevailing situations. An employee can be resilient enough to adapt to the situation and prepare to sail through or fall into the melancholy and sickness of the same. This will lead to the maladaptation stage.
5.3.1.1. Adaptive Strategies
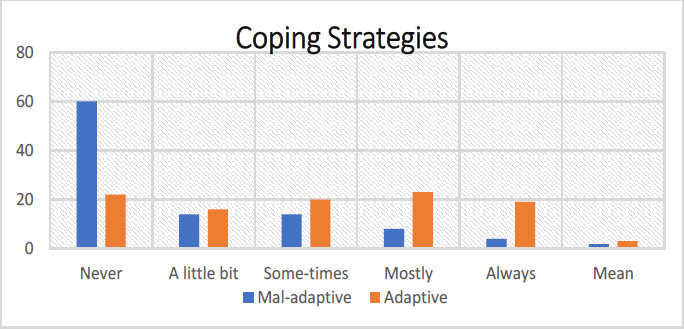
The items include active coping, planning, acceptance, emotional support, humour, positive reframing, and religion. The items or statements included concentrating efforts on doing something about the situation, getting emotional support, taking action to make the situation better, learning to live with it, and comfort in religion or spiritual beliefs. About 42% of the respondents used some adaptive strategies. As many as 38% remained under the never or a little bit zone, thus indicating an inability to adapt to the stressful situation. Table 7 and Fig. (4) depict the responses.
| Construct | Sub-Construct | Never | A Little Bit | Sometimes | Mostly | Always | Mean |
|---|---|---|---|---|---|---|---|
| Coping Strategies (Percentage) | Mal-adaptive | 60 | 14 | 14 | 8 | 4 | 1.81 |
| Adaptive | 22 | 16 | 20 | 23 | 19 | 3.02 |
5.3.2. Mal-adaptive Strategies
The items in the sub-construct include behavioural disengagement, denial, self-distraction, self-blame, and use of substance or venting strategies. The statement capturing these coping mechanisms included, other activities to take the mind off things, saying that ‘this isn’t real’, trying to deal with it, refusing to believe, letting unpleasant feelings escape, using alcohol or other drugs to help, or blaming self for things that happened. The responses are indicative of struggle with 26% of the respondents. However, nearly 74% of the employees were adapting to the new situation and were able to cope with the challenges. The adaptive and maladaptive responses appear to be out of synchrony, reflecting respondents' bias with difficult questions.
5.4. Personal Well-being
Much debated health definition by the WHO [25] highlights the well-being of an individual as, “Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.” Well-being is a wider dimension with many sub-constructs encompassing objective and subjective well-being. The 18-item scale of Ryff and Keyes [26] has six sub-constructs that were studied for the respondents. It sought answers to how well each respondent felt about herself/himself to ascertain the impact of a virus-driven negative environment. The results (Fig. 5) showed a fair percentage of employees struggling to maintain their well-being, which can be flagged as a cause of concern, though the majority of nearly 60% responded well to the environment around them.
5.4.1. The Self-acceptance
The sub-construct looks at personal achievements, self-evaluation, and a feeling of accomplishment. As seen from Table 8, and the figure above, 61% of respondents feel quite satisfied, while 24% struggle to come to terms with accepting themselves. Others are neutral. The average mean value of 3.5 points towards positive self-acceptance.
5.4.2. The Purpose in Life
Statements affirming purpose include using each day well, living for the day, and fulfilling one’s life goals. The number of agreed respondents is 46%. However, if neutral or undecided 23% is included, the majority would fall in the positive mindset. As many as 31% of the respondents feel they are not meeting the purpose in the prevailing situations.
5.4.3. The Environmental Mastery
The ability to manage the environment around and mastery in everyday life constitute this sub-construct. About 56% of the respondents are managing it well, while 20% are fence-sitters. 24% feel that the situation is not conducive to letting them manage the environment around them well.
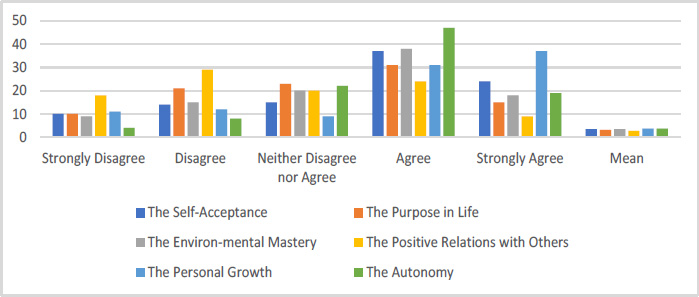
| Construct | Sub-construct | Strongly Disagree | Disagree | Neither Disagree Nor Agree | Agree | Strongly Agree | Mean |
|---|---|---|---|---|---|---|---|
| Personal Well Being (Percentage) | The Self-Acceptance | 10 | 14 | 15 | 37 | 24 | 3.50 |
| The Purpose in Life | 10 | 21 | 23 | 31 | 15 | 3.21 | |
| The Environmental Mastery | 9 | 15 | 20 | 38 | 18 | 3.41 | |
| The Positive Relations with Others | 18 | 29 | 20 | 24 | 9 | 2.76 | |
| The Personal Growth | 11 | 12 | 9 | 31 | 37 | 3.71 | |
| The Autonomy | 4 | 8 | 22 | 47 | 19 | 3.68 |
5.4.4. The Positive Relations with Others
Experience in warm and trusting relationships and the ability to gain and sustain trust are the key items of this sub-construct. This has come out as a major challenge for the respondents in the locked-down conditions with the pandemic situation. Only 33% agree with their abilities to maintain positive and trusting relationships as against 47%, who are doubtful and 20% remain undecided.
5.4.5. The Personal Growth
Continuous learning, taking up challenges and improvement in one’s life figure under this sub-dimension. 68% of respondents agree with these steps, while only 23% have scepticism about the same. Locked-down conditions should have stirred most to acquire new qualifications, add to their skills and continue on a learning path.
5.4.6. The Autonomy
Self-judgement, respecting own opinions and not being unduly influenced by what others say or think were some of the statements depicting individual autonomy. 66% felt they were autonomous, while only 12% considered being influenced by others. As many as 22% did not have any of the extreme views.
A two-stage research process was adopted in the current study. The researchers first used confirmatory factor analysis to validate the measurement model with the help of AMOS. Afterwards, the researcher tested the proposed relationships among the study variables by using the structural equation modelling technique. The data analysis section is subdivided into two parts [27]. The first part deals with the measurement model and the second part deals with the structural model. Under the measurement model, the reliability and validity of the constructs were established and under the structural model, the hypothesized relationships were tested.
5.5. Measurement Model
The value of composite reliability (Table 9) for all the latent variables is higher than 0.70 which is a depiction of higher consistency in the responses of the respondents [28]. The construct validity of the measurement model is established by the two-stage technique [29]. In the first stage, the convergent validity is established and in the second stage, the discriminant validity is established.
For establishing convergent validity, the procedure specified by Fornell & Larcker [29] is followed. The procedure suggests that the value of the standardized regression weight for each statement should be significant and higher than 0.50. Further, the value of average variance extracted (AVE) for each latent variable should be higher than 0.50 and the coefficient of composite reliability for each latent variable (CR) should be higher than 0.70. Finally, the value of CR for each latent variable should be greater than the AVE for each latent variable. The results of Table 9 fulfill all the conditions for establishing the convergent validity. Hence, it can be concluded that the measurement model has good convergent validity.
| Construct | Items | SRW | CR | AVE |
|---|---|---|---|---|
| - | Avoidance 1 | 0.769*** | - | - |
| - | Avoidance 2 | 0.720*** | - | - |
| - | Avoidance 3 | 0.855*** | - | - |
| Avoidance | Avoidance 4 | 0.802*** | 0.944 | 0.678 |
| - | Avoidance 5 | 0.885*** | - | - |
| - | Avoidance 6 | 0.859*** | - | - |
| - | Avoidance 7 | 0.804*** | - | - |
| - | Avoidance 8 | 0.881*** | - | - |
| - | Intrusion 1 | 0.703*** | - | - |
| - | Intrusion 2 | 0.838*** | - | - |
| - | Intrusion 3 | 0.815*** | - | - |
| Intrusion | Intrusion 4 | 0.705*** | 0.930 | 0.626 |
| - | Intrusion 5 | 0.747*** | - | - |
| - | Intrusion 6 | 0.853*** | - | - |
| - | Intrusion 7 | 0.840*** | - | - |
| - | Intrusion 8 | 0.814*** | - | - |
| - | Hyperarousal 1 | 0.779*** | - | - |
| - | Hyperarousal 2 | 0.755*** | - | - |
| Hyperarousal | Hyperarousa l3 | 0.795*** | 0.919 | 0.631 |
| - | Hyperarousa l4 | 0.844*** | - | - |
| - | Hyperarousa l5 | 0.704*** | - | - |
| - | Hyperarousa l6 | 0.876*** | - | - |
| - | DiStress 1 | 0.709*** | - | - |
| - | DiStress 2 | 0.786*** | - | - |
| - | DiStress 3 | 0.763*** | - | - |
| DiStress | DiStress 4 | 0.737*** | 0.910 | 0.590 |
| - | DiStress 5 | 0.772*** | - | - |
| - | DiStress 6 | 0.744*** | - | - |
| - | DiStress 7 | 0.859*** | - | - |
| - | Anxiety 1 | 0.848*** | - | - |
| - | Anxiety 2 | 0.886*** | - | - |
| - | Anxiety 3 | 0.710*** | - | - |
| Anxiety | Anxiety 4 | 0.870*** | 0.921 | 0.627 |
| - | Anxiety 5 | 0.703*** | - | - |
| - | Anxiety 6 | 0.708*** | - | - |
| - | Anxiety 7 | 0.792*** | - | - |
| - | Stress 1 | 0.829*** | - | - |
| - | Stress 2 | 0.793*** | - | - |
| - | Stress 3 | 0.746*** | - | - |
| Stress | Stress 4 | 0.874*** | 0.919 | 0.620 |
| - | Stress 5 | 0.813*** | - | - |
| - | Stress 6 | 0.729*** | - | - |
| - | Stress 7 | 0.715*** | - | - |
| - | Adaptive 1 | 0.760*** | - | - |
| - | Adaptive 2 | 0.731*** | - | - |
| - | Adaptive 3 | 0.837*** | - | - |
| - | Adaptive 4 | 0.714*** | - | - |
| - | Adaptive 5 | 0.758*** | - | - |
| - | Adaptive 6 | 0.841*** | - | - |
| - | Adaptive 7 | 0.705*** | - | - |
| Adaptive | Adaptive 8 | 0.792*** | 0.957 | 0.581 |
| - | Adaptive 9 | 0.761*** | - | - |
| - | Adaptive 10 | 0.767*** | - | - |
| - | Adaptive 11 | 0.708*** | - | - |
| - | Adaptive 12 | 0.736*** | - | - |
| - | Adaptive 13 | 0.757*** | - | - |
| - | Adaptive 14 | 0.758*** | - | - |
| - | Adaptive 15 | 0.761*** | - | - |
| - | Adaptive 16 | 0.792*** | - | - |
| - | MalAdaptive 1 | 0.776*** | - | - |
| - | MalAdaptive 2 | 0.754*** | - | - |
| - | MalAdaptive 3 | 0.757*** | - | - |
| - | MalAdaptive 4 | 0.713*** | - | - |
| - | MalAdaptive 5 | 0.780*** | - | - |
| MalAdaptive | MalAdaptive 6 | 0.740*** | 0.954 | 0.634 |
| - | MalAdaptive 7 | 0.872*** | - | - |
| - | MalAdaptive 8 | 0.837*** | - | - |
| - | MalAdaptive 9 | 0.837*** | - | - |
| - | MalAdaptive 10 | 0.865*** | - | - |
| - | MalAdaptive 11 | 0.787*** | - | - |
| - | MalAdaptive 1 2 | 0.821*** | - | - |
| - | Self-acceptance 1 | 0.847*** | - | - |
| Self-acceptance | Self-acceptance 2 | 0.794*** | 0.833 | 0.626 |
| - | Self-acceptance 3 | 0.728*** | - | - |
| - | Purpose in Life 1 | 0.718*** | - | - |
| Purpose in Life | Purpose in Life 2 | 0.750*** | 0.790 | 0.557 |
| - | Purpose in Life 3 | 0.770*** | - | - |
| - | Environ Mastery 1 | 0.864*** | - | - |
| Environ Mastery | Environ Mastery 2 | 0.870*** | 0.896 | 0.743 |
| - | Environ Mastery 3 | 0.851*** | - | - |
| - | Positive Relations 1 | 0.875*** | - | - |
| Positive Relations | Positive Relations 2 | 0.774*** | 0.875 | 0.701 |
| - | Positive Relations 3 | 0.860*** | - | - |
| - | Personal Growth 1 | 0.767*** | - | - |
| Personal Growth | Personal Growth 2 | 0.711*** | 0.777 | 0.537 |
| - | Personal Growth 3 | 0.720*** | - | - |
| - | Autonomy 1 | 0.835*** | - | - |
| Autonomy | Autonomy 2 | 0.859*** | 0.881 | 0.712 |
| - | Autonomy 3 | 0.837*** | - | - |
When the square root value of an AVE is higher than the correlations between different constructs, discriminating validity is established [30]. The results of Table 10 depict that for all the latent variables, the value of the square root of AVE is greater than its corresponding inter-construct correlation coefficients. Hence, it can be concluded that the present measurement model has achieved discriminant validity (Table 10).
| - | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Avd | 0.823 | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Int | 0.214 | 0.791 | - | - | - | - | - | - | - | - | - | - | - | - |
| Hyp | 0.148 | 0.285 | 0.794 | - | - | - | - | - | - | - | - | - | - | - |
| Dis | 0.114 | 0.045 | 0.112 | 0.768 | - | - | - | - | - | - | - | - | - | - |
| Anx | 0.261 | 0.097 | 0.092 | 0.134 | 0.792 | - | - | - | - | - | - | - | - | - |
| Str | 0.228 | 0.114 | 0.124 | 0.077 | 0.119 | 0.787 | - | - | - | - | - | - | - | - |
| Ada | -0.345 | -0.229 | -0.276 | -0.174 | -0.227 | -0.222 | 0.762 | - | - | - | - | - | - | - |
| Mal | 0.279 | 0.187 | 0.261 | 0.267 | 0.207 | 0.291 | -0.112 | 0.796 | - | - | - | - | - | - |
| SA | -0.254 | -0.336 | -0.244 | -0.165 | -0.117 | -0.116 | 0.254 | -0.111 | 0.791 | - | - | - | - | - |
| PIL | -0.314 | -0.118 | -0.271 | -0.258 | -0.32 | -0.341 | 0.197 | -0.157 | 0.097 | 0.746 | - | - | - | - |
| EM | -0.114 | -0.241 | -0.193 | -0.316 | -0.204 | -0.117 | 0.308 | -0.148 | 0.113 | 0.024 | 0.862 | - | - | - |
| PR | -0.221 | -0.265 | -0.234 | -0.264 | -0.117 | -0.113 | 0.345 | -0.134 | 0.118 | 0.092 | 0.124 | 0.837 | - | - |
| PG | -0.187 | -0.291 | -0.268 | -0.147 | -0.301 | -0.249 | 0.115 | -0.201 | 0.157 | 0.114 | 0.074 | 0.076 | 0.733 | - |
| Aut | -0.305 | -0.154 | -0.112 | -0.302 | -0.124 | 0.302 | 0.208 | -0.208 | 0.075 | 0.098 | 0.176 | 0.087 | 0.085 | 0.844 |
5.6. Structural Model
Structural equation modelling through AMOS 20.0 was used to examine the study's proposed model. The first step in determining the robustness of any model (Fig. 6), according to Hair et al. [27], is to determine whether the model is a good fit or not. The following values illustrate the yardsticks for recommended values as suggested by prior studies for an overall fit. The value of chi-square statistics divided by the degree of freedom is 2.784, which is less than the cut-off value of less than 3. Further, the values of other model fit indices show that overall the proposed model is fit for the analysis as the values of RMR = 0.039 ≤ 0.08, RMSEA = 0.042 ≤ 0.08, CFI = 0.911 ≥ 0.90, AGFI = 0.924 ≥ 0.80, GFI = 0.907≥0.80. Since the model has an acceptable fit, we continued to analyze the path coefficients to test the hypothesis.
| Relationship | SRW | S.E. | C.R. | P | R2 | ||
|---|---|---|---|---|---|---|---|
| Coping | <--- | IESR | -.669 | .015 | -26.310 | *** | .631 |
| Coping | <--- | DAS | -.428 | .010 | -16.827 | *** | |
| PL | <--- | Coping | .431 | .118 | 11.416 | *** | .186 |
| EM | <--- | Coping | .679 | .090 | 22.070 | *** | .461 |
| PR | <--- | Coping | .392 | .087 | 10.173 | *** | .154 |
| PG | <--- | Coping | .632 | .072 | 19.448 | *** | .399 |
| AUT | <--- | Coping | .803 | .061 | 32.199 | *** | .645 |
| SA | <--- | Coping | .051 | .115 | 1.219 | .223 | .003 |
Results of the structural equation modelling technique (SEM) show that there is a significant and negative effect of the “impact of events” factor on the coping strategies of the participants (SRW=-.669; t-value= -26.310; p< 0.05). Hence, hypothesis 1 was accepted. A similar type of result was observed for the relationship between the “depression anxiety and stress” factor and coping strategies factor. Results of Table 11 show that DAS negatively predicts the coping strategies (SRW=-.428; t-value= -16.827; p< 0.05). Hence, hypothesis 2 was accepted. Further, results of the SEM show that coping strategies do not predict the self-acceptance factor (SRW=.051; t-value= 11.2191.416; p> 0.05). Hence, hypothesis 3 was not accepted. The coping strategies have shown a significant positive relationship with the purpose of life (SRW=.431; t-value= 11.416; p< 0.05). Hence, hypothesis 4 was accepted. Further, coping strategies have a significant positive relationship with environmental mastery (SRW=.679; t-value= 22.070; p< 0.05). Hence, hypothesis 5 was accepted. Results of the SEM technique also show that there is a significant and positive effect of the “coping strategies” factor on the positive relations with others (SRW=.392; t-value= 10.173; p< 0.05). Hence, hypothesis 6 was accepted. Results of Table 11 show that coping strategies positively predict personal growth (SRW=.632; t-value= 19.448; p< 0.05). Hence, hypothesis 7 was accepted. Finally, the results of the SEM analysis show that coping strategies have a significant and positive effect on autonomy (SRW=.803; t-value= 32.199; p< 0.05). Hence, hypothesis 8 was accepted.
6. RESULTS & DISCUSSION
6.1. Implications of the Study
6.1.1. Theoretical Implications
The research makes a significant contribution to the validation of existing psychometric scales like IES-R, DASS-21, Coping Strategies Scale, and Personal Well-Being Scale. The high reliability and validity metrics suggest that these scales are robust instruments for studying the psychological impacts of a pandemic or other similar large-scale traumatic events. Further, the study enhances our understanding of the complex interplay between traumatic events, in this case, the COVID-19 pandemic, and various dimensions of mental health, including stress, anxiety, depression, and overall well-being. This sets the stage for future research focused on post-traumatic stress disorder (PTSD) and related psychological conditions. In addition to this, by including the Coping Strategies Scale, the study opens new doors for the investigation of the adaptive and maladaptive coping mechanisms people employ during a crisis. This adds another layer of nuance to trauma and mental health research. Further, given the study's scope and focus, it can act as a bridge between public health policy, organizational behavior, and clinical psychology. This sets a precedent for future interdisciplinary research and encourages holistic approaches to tackling community and workplace well-being. Additionally, given that the study was conducted during a lockdown phase with work-from-home arrangements, the findings offer theoretical insights into how remote working conditions affect employee mental health and coping mechanisms. Finally, this study has the potential to inform theories around crisis management in organizations, particularly regarding employee well-being. Understanding how employees are affected by and cope with large-scale crises could be integrated into theoretical frameworks that guide organizational policies and leadership strategies during times of crisis [31, 32].
CONCLUSION & PRACTICAL IMPLICATIONS
Organizations can use the study’s findings to develop targeted mental health interventions that take into account the specific needs of different demographic groups, thus making support more effective and inclusive. Further, the study's focus on coping mechanisms offers actionable insights for the development of comprehensive employee wellness programs. Workshops or training modules could be designed to educate staff about effective coping strategies during times of crisis. Further, public health agencies may use this study as an empirical foundation to develop or modify policies aimed at enhancing public mental health during pandemics or similar large-scale events. Additionally, insights into the impact of remote working on mental health can be used by companies to tailor their work-from-home policies, perhaps introducing more flexibility or mental health days to better support employee well-being. Further, educational institutions can use these insights to form strategies that address the mental health concerns of students, particularly if they are also working part-time or juggling multiple responsibilities during a crisis. Further, Businesses and other organizations could revamp their crisis communication plans to include components aimed at mitigating psychological stress and enhancing effective coping among employees. This study could help shape legal guidelines around employer responsibilities for employee mental health, particularly during crises like pandemics or natural disasters.
LIMITATIONS OF THE STUDY AND FURTHER SCOPE
Every research comes with some limitations, which should be kept in mind while generalizing the results of the study to the masses. The current study also has a few limitations. It is important to note that the cross-sectional design limits us from drawing any firm conclusions about causal relationships among the study variables. Therefore, future researchers could go for a longitudinal research design so that the causal relationship among the variables could be established. Another limitation is related to the data. As the data was collected from university staff, the results of the current study may not be applicable to other sectors. Hence, future researchers could include more sectors such as manufacturing or IT industry to enhance the generalizations of the results. While our (confirmed) model was built on theory and prior empirical research, further testing using a longitudinal design is warranted. Another limitation is related to response bias. Due to the self-report nature of the study, it was not possible to eliminate response bias even if respondents completed the surveys anonymously. In the future, the researchers should try to replicate the findings using more robust samples.
AUTHORS' CONTRIBUTIONS
The first author compiles research designs, collects data, conducts theoretical studies, and compiles research drafts. The second author is the corresponding author, doing literature reviews, analyzing and interpreting data, and performing proofreading. The third author contributes to compiling research questionnaires and collecting data. The fourth author contributes to the introduction, research design and discussion.
ABBREVIATION
| (PWB) | = Psychological Wellbeing |
ETHICAL STATEMENT
The study design and protocols were approved by the Internal Ethics Committee of Chitkara University, India.
CONSENT FOR PUBLICATION
Consent to participate in this study was indicated by respondents.
AVAILABILITY OF DATA AND MATERIALS
The data that support the findings of this study can be made available to qualified researchers from corresponding authors [A.A] upon reasonable request.
FUNDING
None.
CONFLICT OF INTEREST
Dr. Amit Mittal is the Associate Editorial Board Member for The Open Psychology Journal.
ACKNOWLEDGEMENTS
Declared none.

