All published articles of this journal are available on ScienceDirect.

Successful Aging Among a Sample of Iranian Older Adults
Abstract
Background:
Successful Aging (SA), as one of the most important indicators of elderly people's health, has received substantial attention in the gerontological literature.
Objective:
The present study aimed to identify the successful aging status and its associated factors.
Methods:
A cross-sectional study was conducted using the stratified multistage sampling method. In 2015, a total of 600 community-dwelling participants aged 60 years or older in Tehran participated in this study. The SA was measured by a validated questionnaire consisting of seven dimensions. A Stepwise multiple linear regression analysis was done using SPSS to identify the most important predictors of SA.
Results:
The mean age of the participants was 69.7 (SD=7.5), and around 46% of them were retired. The mean score of the composite index of the SA was 65.6 (SD=10.8; expected range 0-100). The results of the study showed that 11.2% of the participants were aging successfully. The results of the stepwise multiple linear regression analysis revealed that childhood health status, socioeconomic status in childhood, level of education, marital status, income, and the number of diseases are significantly contributed to successful aging.
Conclusion:
The results of the present study showing only a few of the participants are aging successfully, imply that social and health policymakers must pay more attention to the aging population, particularly those with low social status and chronic medical status.
1. INTRODUCTION
The population aging in all societies will result in profound changes in the economic, social, and political sectors [1]. For this reason, several studies have been conducted to overcome the challenges caused by such profound changes in micro and macro levels [2]. One of the key concepts in these studies dealing with the problems of population aging, would be the concept of Successful Aging (SA). At first glance, the combination “successful” and “aging”, which together makes the phrase “successful aging”, seems an oxymoron, because “aging” is
normally associated with loss or approaching death, while “successful” is usually related to the concepts of win and development [3]. The phrase “successful aging” may present a superficial contradiction, but the meaning of “success” in the aging period would be completely different from its meaning in other periods of one's life [3]. The phrase “successful aging” was first defined by Robert Havighurst in 1961, meaning a feeling of happiness and satisfaction [4].
In the last decades, various models of successful aging have been proposed by researchers both for defining and measuring it. Three classical theories, such as “Activity Theory”, “Disengagement Theory”, and “Continuity Theory” [5], derived from “functionalism approaches”, were related to these models [6]. In the literature of SA, two well–known models are more operative. The first model is called “Rowe & Kahn Model” in which the SA is separated from the normal aging considering three different dimensions such as ” lack of the disease and disability”, “the high physical and cognitive functioning”, and “the role of engagement with life” [7]. The second model is called “SOC”, which was proposed by Baltes and Baltes in 1990. This model has three factors, including Selection, Optimization, and Compensation. They are essential for successful development regarding the maintenance of functioning and the minimization of losses. In this model, successful aging includes a selection of functional domains, which focuses on one’s resources, optimization of developmental potential and aids that facilitate success and compensation for losses or proactive coping [3, 8].
Modern theories emphasize on the subjectivity of the concept of the SA, such as the theory of “Gerotranscendence” combining “growth” and “activity” in old age defining the elderly’s “transcendence” in connection with the “self” and “ontology” [9], or the theoretical framework of “Culturally–relevant” centering on the cultural context of SA [10].
In the literature, the SA concept is considered as a process and an outcome. Erikson's “Theory of Growth” has a significant role in clarifying and defining “success” as a process of aging. According to the Erikson's psychological theory of growth, “generativity” in middle age would be considered as the basis for “aging well” [11]. Moreover, other models such as Schulz and Heckhausen's “Life Span” considered successful development as a lifelong adaptation from infancy to old age and present their model from a life course perspective [12].
According to the life course approach, aging well depends on the developmental process and early environmental influences [13]. There are critical periods of growth and development during childhood and adolescence in which ecological exposures do more damage to long-term health. WHO emphasized that social and geographical inequalities have a major role in the distribution of chronic disease. Socio-economic status throughout the life- course determines illness risk and old age health [14]. Then, childhood circumstances such as mistreatment and low Socio-Economic Status (SES) of the family may contribute to the chronic disorders in later life [15, 16]. There is an argument that “high SES” in adulthood might moderate the negative effect of poor SES in childhood on later-life health [17]. Table 1 shows a summary of successful aging models and theories.
There are two viewpoints on measuring SA. In the first perspective, dichotomizing successful versus usual elderly people (binary modeling) based on the cut-off criteria of objective physical and mental tests [18, 19]. In the second perspective, success was indicated as a spectrum and subjective concept (continuum-based measure) measured based on the self-appraisal of laypersons’ perception [20-22]. In the present study, the holistic and multidimensional continuous concept of SA derived from the second viewpoint was represented
In Iran, since baby boomer generation entered the aging period, the phenomenon of the population aging will occur after 2050. Based on the 2016 census, at present, 9.3 percent of the Iranian population aged 60 years and older [23]. To manage the challenges of population aging, monitoring older adults based on the index showing the status of multidimensional health is required. The appropriate SA approach with the main focus on the life-course perspective can help policy–makings. Thus, the present study aimed to assess the status of Iranians’ successful aging and its associated factors.
| Definition or Dimensions | Authors (Year) | Main SA Models or Theories |
|---|---|---|
| Integrity Vs. Despair Based on Generativity stage of midlife | Erikson(1950) | Erikson development theory |
| withdrawal or disengagement from the interaction between the individual and her/his social context | Havighurst and Albrecht(1953); Lemon, Bengston and Peterson (1972) |
Disengagement Theory |
| life satisfaction is positively related to social integration and high involvement with social networks | Cumming and Henry (1961) | Activity Theory |
| Try to preserve the habits, preferences and favored lifestyle acquired over a lifetime as long as possible. | Atchley, 1999 | Continuity Theory |
| Selection, Optimization and compensation | Baltes & Carstensen (1996) |
SOC model |
| lack of the disease and disability, the high physical and cognitive functioning, engagement in life/social participation |
Rowe & Kahn(1997) | Rowe & Kahn Model |
| Lifelong adaptation and developmental regulation from infancy to old age. The model included development and maintenance of primary or secondary control throughout the life course | Schulz & Heckhausen(1996) | Life Span |
| Value orientations such as Human nature, Man-nature, Relations, Time, activity | Torres(1999) | culturally-relevant Successful aging |
| Self-transcendence(decrease in self-centeredness and a decline in material), relationship(need for solidarity), cosmic (redefinition of life and death) | Tornstam, 2005 | Gerotranscendence |
2. METHODS
2.1. Participants and Data Collection
This cross-sectional study was conducted on 600 community-dwelling participants aged 60 years or older in Tehran. They were selected by the multistage stratified sampling method in 22 districts of Tehran. In each district, two neighborhoods were randomly chosen. Then, three blocks were selected in each neighborhood and older adults living in those blocks were interviewed. Data were collected using a face- to- face interview by trained enumerators in respondents' homes after getting informed consent from all participants. This study has been approved by the Research Ethics Committee of the University of Social Welfare and Rehabilitation Sciences.
2.2. Measurements
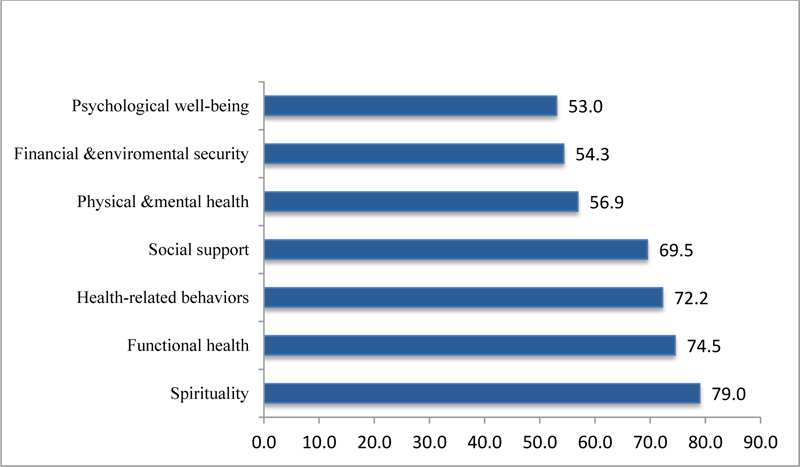
In the current study, to measure self-perceived successful aging as a dependent variable, a validated instrument (SSAI) was developed based on the qualitative interview with Iranian older adults as well as an integrative review of the research background [24]. SSAI has 54 items and seven sub-scales including “the psychological well-being”, “the social support”, “the financial-environmental security”, “functional health”, “physical and mental health”, “health-related behaviors” and “spirituality”. The SSAI had a high internal consistency (Cronbach’s alpha=0.93).
To compare dimensions of successful aging, each dimension has been standardized in the range of 0 to 100. The composite index of SA was composed of seven equally weighted dimensions. A higher score represents a higher value of SA. The mean score of the composite index of the SA obtained by the participants was 65.6(SD= 10.8); 11.2 percent of participants obtained the 80th percentile or higher on the SA scale which shows they could get successful aging [25].
Childhood socioeconomic status and health status = were assessed by two questions including “what was your family’s socioeconomic situation during the first 15 years of your life?” and “how was your health status during the first 15 years of your life?”
Moreover, demographic variables included sex (0= male, 1= female), age at interview, Marital status (0= Widowed/divorced, 1= married), Education (0= illiterate, 1= Primary, 2= Secondary, 3= Higher education), Employment status (1= employed, 2= retired 3= Housewife), living status (0= alone, 1= Living only with children, 2= Living only with spouse, 3= living with spouse & children), Household income (1= Less than $300, 2=$301-600, 3=$601-900, 4= More than $900), Neighborhood SES (1= low, 2= middle, 3= high), Number of diseases (0=no diseases, 1=One diseases, 2=2-3 diseases, 3=4-5 diseases, 4=6+ diseases).
2.3. Analytical Strategy
Data analysis, including descriptive and inferential statistics, were conducted using SPSS 20.0. The descriptive statistics such as percentage, frequency, and mean were conducted to illustrate the characteristics of the study sample. The inferential statistics, such as bivariate analyses and Stepwise multiple linear regression were done to discover relationships among the study variables.
3. RESULTS
The results of the present study showed that around 51 percent of the samples were older women (Mean age=69.7, SD= 7.5), about 46% retired, 16.2% employed, 75% married, and 16.5% had no formal education (Table 1).
3.1. Successful Aging and Its Dimensions
Fig. (1) displays the mean score of the dimensions of the SA. Based on the results of the present study, the highest mean score of the participants goes to spirituality and functional health dimensions while the lowest mean score goes to the psychological health and financial- environmental security, respectively.
3.2. Bivariate Analysis
Table 1 shows the association among each of the demographic variables, childhood health status and childhood perceived SES with the index of SA. The results revealed a significant association between the SA index and the variables of age, marital status, education, employment status, living arrangements, household income, Neighborhood SES, number of diseases, childhood health status, and perceived childhood SES.
3.3. Stepwise Multiple Linear Regression Analysis
As the results presented in Table 2, stepwise multiple linear regression analysis was conducted to determine significant predictors of the successful aging index. The results of stepwise multiple linear regression analysis revealed that the number of diseases, education, marital status, childhood health status, childhood perceived SES, and household income significantly contribute to successful aging index.
| Variable Category | % | Mean | SD | F / t | p-value | |
|---|---|---|---|---|---|---|
| Age Groups | Young Old | 53.8 | 66.8 | 10.4 | 8.27 | P<0.001 |
| old | 32.5 | 65.5 | 10.8 | |||
| oldest old | 13.7 | 61.4 | 11.7 | |||
| Sex | men | 48.8 | 66.0 | 10.4 | 0.835 | p=0.404 |
| women | 51.2 | 65.3 | 10.8 | |||
| Marital status | widowed/divorced | 25.0 | 61.2 | 11.0 | -5.805 | P<0.001 |
| married | 75.0 | 67.1 | 10.3 | |||
| Education | illiterate | 16.5 | 59.3 | 11.6 | 22.865 | P<0.001 |
| primary | 49.2 | 65.3 | 8.9 | |||
| secondary | 21.8 | 67.9 | 11.5 | |||
| higher education | 12.5 | 71.6 | 11.1 | |||
| Employment status | employed | 16.2 | 66.2 | 10.8 | 0.726 | p=0.484 |
| retired | 46.3 | 66.0 | 11.8 | |||
| housewife | 42.2 | 65.0 | 9.7 | |||
| living arrangement | alone | 16.1 | 60.5 | 11.4 | 14.210 | P<0.001 |
| only with children | 7.7 | 61.1 | 10.5 | |||
| only with spouse | 44.0 | 66.8 | 9.6 | |||
| with spouse and children | 32.2 | 67.7 | 11.2 | |||
| Household income per month |
< $ 300 | 17.7 | 60.61 | 10.6 | 10.590 | P<0.001 |
| $301-$600 | 51.7 | 65.64 | 9.9 | |||
| $601-$900 | 14.9 | 68.56 | 11.0 | |||
| > $900 | 15.7 | 68.44 | 11.9 | |||
| Neighborhood SES | high | 24.3 | 65.97 | 11.7 | 12.390 | P<0.001 |
| middle | 18.0 | 67.91 | 9.3 | |||
| low | 22.0 | 62.79 | 11.1 | |||
| Number of diseases | 0 | 9.4 | 72.21 | 9.6 | 23.533 | P<0.001 |
| 1 | 15.7 | 70.36 | 10.0 | |||
| 2-3 | 37.0 | 66.54 | 10.3 | |||
| 4-5 | 26.8 | 61.98 | 10.4 | |||
| 6+ | 11.2 | 59.14 | 9.4 | |||
| Perceived SES of childhood |
low | 28.9 | 62.28 | 11.9 | 32.924 | P<0.001 |
| middle | 49.6 | 66.01 | 9.8 | |||
| high | 21.5 | 69.32 | 10.3 | |||
| Perceived Childhood health status |
bad | 11.2 | 63.04 | 8.0 | 19.329 | P<0.001 |
| fair | 24.8 | 61.64 | 9.5 | |||
| good | 64.0 | 67.72 | 11.3 | |||
| Predictors | b | Beta | t |
|---|---|---|---|
| Number of Diseases | -3.139 | -0.266 | -7.120*** |
| Education | 2.014 | 0.163 | 3.930*** |
| Childhood Health | 2.744 | 0.173 | 4.785*** |
| Marital status(unmarried®) | 3.641 | 0.145 | 3.927*** |
| Childhood SES | 2.336 | 0.153 | 4.168*** |
| Income | 0.63 | 0.103 | 2.521* |
* p≤0.05, ** p<0.01, ***p<0.001
The regression equation predicts six of the eleven successful aging determinants. The value of R-squared indicates that almost 28 percent of the variance in the score of the composite index of successful aging can be explained by predictors. Among these predictors, the number of diseases had the strongest effect on the successful aging index Table 3.
4. DISCUSSION
The present study was conducted on 600 Iranian community-dwelling older adults to determine SA status and its associated factors in 2015. The results of the study revealed that 11.2 percent of participants feel aging well. According to the systematic review by Depp and Jest (2006), the prevalence of SA ranged from 0.4% to 95% [26]. Further, Cosco et al., (2014) presented the prevalence of SA from 0.4% to 91.7% [18]. This wide variation is caused by a variety of subjective and objective definitions of successful aging as well as single or multi-criteria measurements. Cernin et al. (2011) compared self-rated SA and successful aging based on objective criteria and revealed a discrepancy between self-rated and objectively defined success. About two-thirds of the sample rated themselves as successful elderly, whereas only around 30% of the sample met MacArthur objective criteria [19]. The results of the present study provide evidence for multidimensional approaches, and few participants achieved successful aging.
The results of the inferential statistics showed that married older adults, elderly with a higher level of education and income, and participants with a lower number of diseases have a higher score of SA. Further, the elderly from higher socio-economic status during childhood as well as better childhood health status had a higher score of SA.
The number of diseases had the most potent effect on the successful aging index. The results of the present study are consistent with those of several studies which found that self-perceived successful aging is associated with an increase in medical comorbidity [27].
Also, previous studies revealed that the individual's level of education and income are factors that affect aging well [28]. According to “Fundamental Cause Theory,” which focuses on the individual's risk factors, regardless of the social structure, the inequality of health may not be decreased in a long period [29]. Thus, the evidence point to the importance of focusing on disparities in the social structure for eliminating inequality in SA [28]. Those educated and wealthy older adults living in developed regions access social opportunities and facilities better. Thus, to reduce health inequality, social protection planning should focus on supporting the lower–class older adults of society.
Socioeconomic (income, education, and employment) advantages/disadvantages accumulated throughout life cause morbidity inequalities in old people [30]. The results of the present study are consistent with the theory of “Life-course” which focuses on the inequalities accumulated over the life course, pointing to the effect of childhood circumstance on aging well [29]. Thus, the level of socio-economic status, especially having a sufficient salary, the government's financial support, or having personal properties are considered as basic factors with positive effects on successful aging in developing countries [31, 32].
Considering “marital status” factor, undoubtedly, the factor of “married life” plays a significant role in successful aging. In most studies, the existence of the familial and social supporting system as a stress-buffering has been emphasized by elderly people [21, 33]. According to Fry et al. (2007), different cultures and perceptions will bring different reactions to elderly people who seek SA. They show that in eastern societies, the SA is defined by the elderly person's family and social relationships. The factor of social relationships increases the open-mindedness and resiliency of older adults. On the contrary, in western societies such as the United States of America, the factors of activity, participation, and the feelings of vitality are closely intertwined with successful aging [34].
Although in previous studies, “sex” was considered as one of the significant variables on aging well [26, 35, 36], the sex differences were not significant in the present study. The elderly female’s lowness of average score may be caused by other variables such as the marital status as well as the level of education status. However, in other studies, the predictor of sex loses its significant relation with successful aging in the Multiple regression analysis [37, 38].
CONCLUSION
In summary, SA is a continuous multidimensional concept including the individual's resources (the individual's psychological well-being, the mental and physical health, the functional health, the health-related behaviors, parentheses the compensatory/ protective buffer (the “social support” and “spirituality”) and the age-friendly context (the “economic- environmental security”). Considering the low mean score of psychological well-being and financial- environmental security in Iran, national social welfare policy, entertaining programs, and public pensions’ coverage must be implemented. Moreover, investigating the determinants of the SA index indicated that vulnerable groups of elderly (such as unmarried older adults with low levels of education and income, low SES and health status during childhood as well as experiencing elderly comorbidity) need more attention in the social protection policy.
LIMITATIONS AND SUGGESTIONS
Considering the limitations in the cross-sectional study, we were unable to investigate the causal effect of determinants such as childhood circumstances on aging well. Moreover, this study was carried out on community-dwelling older adults; so it is suggested that the SA index discover older people living in rural or nursing homes and did not enjoy some factors of the SA, such as the familial support. Furthermore, the SA index and its compensatory mechanisms among minority groups of older people, such as disabled elderly or ethical groups are under question and require deep investigation. Moreover, it is suggested to measure the composite index of the SA based on SSAI for investigating the effect of different cultures and societies on SA dimensions.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study has been approved by the Research Ethics Committee of the University of Social Welfare and Rehabilitation Sciences Tehran,Iran. (USWR.REC.1393.135).
HUMAN AND ANIMAL RIGHTS
Not Applicable.
CONSENT FOR PUBLICATION
Informed consent was taken from all the participants when they were enrolled.
AVAILABILITY OF DATA AND MATERIALS
The data that support the findings of this study are available from the corresponding author [Y.A.M] upon request.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Thanks and appreciation were given to all participants.

