All published articles of this journal are available on ScienceDirect.

Substances led to Psychosis: A Systematic Review
Abstract
Background
Psychosis is one of the mind-related disorders that has been common in the new generation, and it has an increasing trend. Psychosis is a variable feature of mood that could be a result of substance use, which includes a few psychiatric and neurologic symptoms. Common symptoms of psychoses are delusions, hallucinations, disorganized thinking, grossly disorganized, or abnormal motor behavior. An array of illicit substances and drugs that can lead to psychosis include cannabinoids, cocaine, amphetamines, methamphetamines, alcohol, etc.
Objectives
The main aim of this review was to discover, analyze, and combine the information concerning substances that could potentially cause psychoses.
Methods
We conducted a literature search on the following network databases: PubMed, Scholar, Science Direct, PubChem, Scopus, and Web-Of-Science. We selected 14 studies potentially relevant articles published from 1990 to 2023 for detailed evaluation. The systematic review was done adhering to PRISMA guidelines. We gathered the important primary studies of eligible systematic reviews and collected data on the interventions employed in these studies to comprehend the strategies that were pursued.
Results
Our result indicated that there are a few substances, which include Cannabinoids, Alcohol, Amphetamine, Cocaine, Nicotine, Kratom, Cathinone, etc., that may lead to psychoses with average to high possibility.
Conclusion
Evidence regarding frequently encountered substances that might contribute to psychosis presents an opportunity to develop customized interventions in the form of user-friendly menus aimed at meeting individuals' requirements and urging them to refrain from consumption.
1. INTRODUCTION
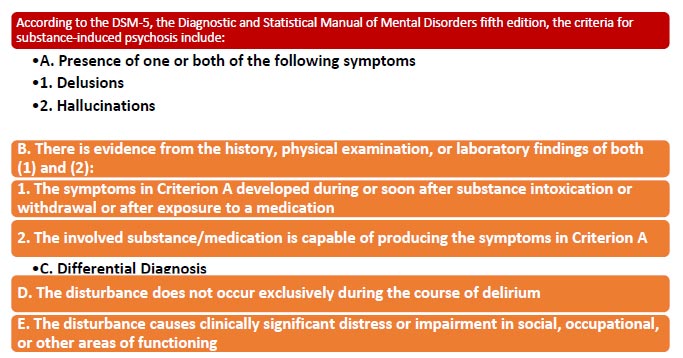
Experimental data indicate diverse subgroups of individuals diagnosed with various severe psychiatric disorders, such as new-onset psychosis and substance-induced psychosis, frequently exhibit abnormalities. These abnormalities commonly manifest in clinical practice [1]. Psychosis is one of the mind-related disorders that has been common in the new generation, and it has an increasing process [2]. Psychosis is an inconstant feature of mood that could be an outcome of substance use, which includes a few functionally psychiatric and neurologic symptoms. In the initial version of the Diagnostic and Statistical Manual of Mental Disorders (DSM), psychosis was described as ” abnormalities in one or more of the following five domains: delusions, hallucinations, dis- organized thinking speech, grossly disorganized or abnormal motor behavior, and negative symptoms” or “gross impairment in reality testing” that interferes with the capacity to meet the ordinary demands of life [3] (Fig. 1). There are a few kinds of substances and drugs that can lead to psychosis; however, the reasons for this association. A clear connection between drug use and the appearance of psychotic symptoms has received considerable backing. Some studies indicate that drugs like cannabinoids, cocaine, amphetamines, methamphe- tamines, alcohol, methylphenidates, nicotine, Kratom, hallucinogens, and certain antibiotics possess psycho- tomimetic properties. [4]. Also, drug abuse has been one of the most popular behaviors in the new generation, and the chemical formula of psychoactive drugs is progressing. Thus, it is probable that substance-induced psychosis may become a pandemic in the future [5]. This review aimed to find, analyze, and summarize the information on substances that could cause psychoses. In other words, it may cause temporary psychotic symptoms as a result of immediate intoxication and psychotic disorders [5, 6]. In another hand, it has been strengthened by teenagers [7-11]. The research gaps of recent articles are limited focus on specific substances, Insufficient research on longitudinal effects, variability in study methodologies, lack of research on specific populations, limited exploration of underlying mechanisms, and Sparse data on effective interventions. Therefore, these potential research gaps could provide avenues for future research to deepen our understanding of the relationship between substances and psychosis; the aim of this article is to resolve these research gaps.
| Authors | Year | Title | Focus | Sample | Main Results |
|---|---|---|---|---|---|
| Fiorentini, Alessio; Sara Volonteri, Lucia; Dragogna, Filippo; Rovera, Chiara; Maffini, Michele; Carlo Mauri, Massimo; A. Altamura, Carlo [1]* | 2011 | Substance-Induced Psychoses: A Critical Review of the Literature | Drugs that may lead to psychoses | 23 | Most of the drugs, such as cannabinoids, may lead to psychoses. |
| Dharav Shah, Prabhat Chand, Mrunal Bandawar, Vivek Benegal, Pratima Murthy [75]* |
2017 | Cannabis-induced psychosis and subsequent psychiatric disorders | Cannabis and psychoses | 38 | Cannabis may lead to psychoses. |
| Vera L. Alves,João L. Gonçalves,Joselin AguiarCQM – Centro de Química da Madeira, Universidade da Madeira, Funchal, Portugal;,Helena M. Teixeira &José S. Câmara [74]* | 2020 | The synthetic cannabinoids phenomenon: from structure to toxicological properties. A review | Synthetic cannabinoids and psychiatric disorders | 42 | Synthetic cannabinoids can considerably lead to psychoses. |
| Anna Sunshine, Jon McClellan [3]* | 2023 | Practitioner Review: Psychosis in children and adolescents | Psychoses in children | 58 | Drug use by children can lead to psychosis. |
| F. Schifano, F. Napoletano, S. Chiappini, A. Guirguis, J. M. Corkery, S. Bonaccorso, A. Ricciardi, N. Scherbaum And A. Vento [4]* |
2019 | New/emerging psychoactive substances and associated psychopathological consequences | New drugs and psychiatric disorders. | 66 | Future drugs lead to psychotic symptoms. |
| Hannah E. Brown, Yoshio Kaneko & Abigail L. Donovan [6]* | 2019 | Substance-Induced Psychosis and Co-occurring Psychotic Disorders | Psychosis because of drug use such as cocaine, etc. | 87 | Amphetamine and cocaine considerably can lead to psychoses. |
| NEUFELD, NICHOLAS H. MD; MOHAMED, NOURHAN S. MD; GRUJICH, NIKOLA MD; SHULMAN, KENNETH MD [45]* | 2017 | Acute Neuropsychiatric Symptoms Associated with Antibiotic Treatment of Helicobacter Pylori Infections: A Review | Antibiotics as a risk factor for psychiatric patients. | 91 | Antibiotics may lead to psychoses. |
| Pedro Gurillo, MD, Dr. Sameer Jauhar MRCPsych, Robin M Murray FRS, James H MacCabe, FRCPsych [9]* |
2015 | Does tobacco use cause psychosis? Systematic review and meta-analysis | Smoking and psychosis | 94 | Nicotine may be a factor that increases the incur of psychosis |
| M.C. Cancino Botello, M.D.L.A. Canseco Navarro, A. Peña Serrano, F. Molina López and J.M. Hernández Sánchez [38]* |
2020 | Psychosis, cause or consequence of substance use disorder | Drug use and psychotic symptoms | 102 | Drugs lead to psychotic symptoms considerably. |
| M.C. Mauri a, C. Di Pace a, A. Reggiori a, S. Paletta a, A. Colasanti [12]* | 2017 | Primary psychosis with comorbid drug abuse and drug-induced psychosis: Diagnostic and clinical evolution at follow up | Substance abuse and psychiatric disorders. | 108 | Substance abuse lead to psychotic symptoms. |
| Corinne Cather, Gladys N. Pachas, Kristina M. Cieslak & A. Eden Evins [21]* | 2017 | Achieving Smoking Cessation in Individuals with Schizophrenia: Special Considerations | Smoking as a risk factor for psychotic patients. | 157 | Smoking may lead to psychoses in a long-term use. |
| L. R. Valmaggia , F. L. Day, C. Jones , S. Bissoli, C. Pugh , D. Hall, S. Bhattacharyya , O. Howes, J. Stone , P. Fusar-Poli, M. Byrne And P. K. McGuire [76]* |
2014 | Cannabis use and transition to psychosis in people at ultra-high risk | Cannabinoids and psychoses | 198 | Cannabinoids may strongly lead to psychoses. |
| Khadija Pasha, Salomi Paul, Muhammad S. Abbas, Sondos T. Nassar, Tasniem Tasha, Anjali Desai , Anjana Bajgain, Asna Ali, Chandrani Dutta, Abeer O. Elshaikh [23]* |
2023 | Psychosis Induced by Methylphenidate in Children and Young Patients with AttentionDeficit Hyperactivity Disorder |
Methylphenidate and psychosis | 202 | Methylphenidate leads to psychotic symptoms. |
| G. Martinotti1 , M. Di Nicola2 , D. Quattrone1 , R. Santacroce1 , F. Schifano, R. Murray4 , M. Di Giannantonio1 [64]* |
2015 | Novel psychoactive substances and induced phenomena in psychopathology: the lysergic psychoma |
psychotic symptoms by drug use | 212 | Methamphetamine, Amphetamine, methylphenidates, etc., can lead to psychoses. |
2. MATERIALS AND METHODS
The databases include PubMed, Scholar, Science Direct, PubChem, Scopus, and Web-Of-Science. The steps involved in conducting this systematic review are
1-Formulating the research question (Clearly defining the research question “Which substances may lead to psychoses?” or hypothesis “Most of the usual drugs and some Antibiotics may lead to psychoses.” that the systematic review aims to address)
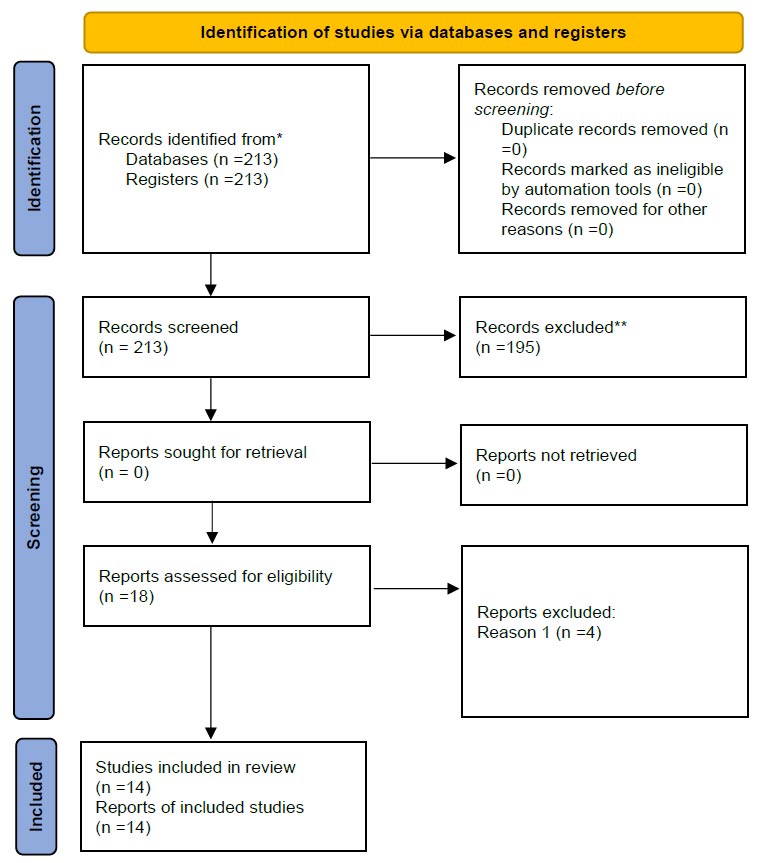
2-Developing inclusion and exclusion criteria (Setting specific criteria for including or excluding studies based on relevance and quality. The inclusion criteria include all clinical studies concerning adult (more than 17 years old) patients, published in English, content directly relevant to substance-induced-psychosis, report original patient, and studies defining drugs that can be related to psychosis.Exclusion criteria include studies with less than 10 participants, case reports, animal studies, articles that were not available in English, content related to other disorders like schizophrenia, not concerned with the field of substance-induced-psychosis, repeated research, unavailable full research (Tables 1 and 2), 3-Systematic search for studies (Conducting a comprehensive and systematic search across multiple databases such as PubMed, Scholar, and Science Direct, PubChem, Scopus, and Web-Of-Science to identify all relevant studies), 4-Screening and selecting studies (Reviewing titles, abstracts, and full texts of potentially relevant studies to determine which ones meet the inclusion criteria. We focused on review articles for our results. If the database did not have that filter, we looked for search terms related to reviews (like Review, systematic review, and meta-analysis) in our search strategy. Our main search topics were 'substance use and psychosis' and 'psychological intervention' (including psychological symptoms and behavior therapy, for instance) (Fig. 2). 5-Data extraction (Extracting relevant data from each included study using a predefined data extraction form), 6-Quality assessment (Assessing the quality of included studies to evaluate their risk of bias and methodological rigor), 7-Data synthesis (Analyzing and synthesizing the findings of the included studies using narrative synthesis which involves summarizing and qualitatively analyzing the findings of individual studies to identify patterns, themes, and discrepancies and qualitative thematic analysis methods to identify and interpret recurring themes, patterns, or discrepancies across the included studies. This can enrich the understanding of complex phenomena), 8-Interpreting results (Drawing conclusions based on the synthesized evidence and discussing implications).
3. RESULTS
3.1. Eligible Reviews
The search of the databases has returned 213 references. After excluding 116 duplicates based on title, we screened the titles of 97 studies. After excluding 79 duplicates based on abstract, we screened abstracts of 18 studies. We managed to obtain 14 complete texts. Fig. (1) summarizes the screening process described above. The reviews that were included had differences, as outlined below. Our research has found 14 studies examining the relationship between substance use and psychosis. Although the methodologies of studies and substance use psychosis criteria have varied, there was a considerable consistency between substance use and psychosis.
3.2. Conceptualization of Substance-induced Psychosis (SIP) in the Eligible Reviews
The current research findings have provided insight into the intricate connection between psychotic symptoms and the utilization and misuse of illegal substances. Moreover, there are instances where chronological factors alone are inadequate to establish a clear cause-and-effect connection between the substances and psychosis. To determine if psychotic symptoms in individuals with a history of drug use are truly independent of the drugs, these symptoms must persist even after a prolonged period of abstaining from psychoactive substances. It's worth noting that drug-induced psychosis is generally expected to resolve during a period of abstinence. People with drug-induced psychosis, in contrast, had a higher tendency to abuse multiple drugs and appeared to experience prolonged hallucinations even after stopping drug use [12].
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| • All clinical studies concerning adult (more than 17 years old) patients • Published in English • Content directly relevant to substance-induced-psychosis • Report original patient • Studies defining drugs that can be related to psychosis |
• Studies with less than 10 participants • Case reports • Animal studies • Articles which were not available in English • Content related to other disorders like schizophrenia, not concerned with the field of substance-induced-psychosis • Repeated researches • Unavailable full researches |
3.3. Cannabinoids
In 2019, cannabinoids were the most commonly used illegal substance, with 22.2 million adults in Europe having used cannabis [13]. The point is that the effect of cannabis is related to its tetrahydrocannabinol (THC) content. THC causes negative effects associated with cannabis, such as cognitive impairments and the promotion of psychosis and anxiety [14]. This receptor is mainly found on peripheral nerve terminals. Cannabidiol (CBD) appears to be the second most prevalent cannabinoid that does not seem to cause any signs of psychosis. Marijuana includes 20% THC, and its concentrates include hash oil, wax, and edibles containing 60% THC [15-18] (Table 3).
3.4. Alcohol
Alcohol has a main role in substance use disorder, and alcohol-use disorders are associated with a considerable burden in terms of morbidity and mortality [19]. Psychotic symptoms can occur in several clinical conditions that are related to alcohol use and can lead to first-episode psychosis as well ref. Despite the main role of alcohol in substance use disorders, recent studies on substance-induced psychotic disorders have generally shown psychoses are usually induced by illicit drug use. Alcohol-induced psychotic disorder is a severe mental disorder with poor outcome [20]. However, the point is that it can be cured by behavior therapy with considerable outcomes (Table 3).
3.5. Nicotine
Nicotine is one of the most popular substances that has been used by a large group of people, especially young generations. It is the basic substance used to make cigarettes, and it comes from tobacco, which is a plant. Usually, people smoke cigarettes during adolescence, so there can be a huge misuse by individuals, and it has been associated with an increased risk factor of psychosis REF. Also, genetics may influence this association as genes associated with psychosis have been shown to overlap with those for cigarette smoking ref. It also increases cytochrome CYP1A2 enzyme activity, so it increases metabolism in a way [21]. Behavioral therapy can be useful even more than medicine in quitting smoking (Table 3).
| Substance | Antidote | Exposure | Treatment | Symptoms | Neurotransmitter/pathways/receptors Implicated | Chemical Structure |
|---|---|---|---|---|---|---|
| Cannabinol | Naloxone (97) | Oral, inhaled. (35) | Decreasing THC levels in cannabis leads to decreasing the risk factor of psychotic disorder even for daily users(34) | Reducing the level of THC in cannabis lowers the likelihood of developing a psychotic disorder, even for individuals who use it daily. (36) |
They influence the endocannabinoid system, specifically by fully activating CB1 and CB2 receptors. |
 C21H26O2 |
| Alcohol | Metadoxine, Fomepizole | Drink(self-use and used by moms) | Behavioral therapy | Visual illusion, nauseous, loss of regular movements | - |
 C2H6O |
| Nicotine | Benzodiazepines, Atropine, Ventilator, Intravenous fluids | Inhalation, insufflation, oral, rectal. |
Medical care, behavioral therapy | - | - |
 C10H14N2 |
| Amphetamine (psychostimulant) | Benzodiazepines (98) | Oral (self-used by youth) | Medical care and do not misuse | Serotoninergic syndrome, Psychosis, Paranoid ideation, Impulsivity, Mania, Agitation, | Mood disorders like serotonin syndrome (Serotoninergic syndrome), psychosis, paranoid thoughts, impulsive behavior, manic episodes, and agitation are commonly associated with the use of psychostimulants. These drugs traditionally focus on activating the monoaminergic systems, resulting in higher levels of serotonin (5-HT), dopamine (DA), and/or norepinephrine (NA) C9H13N Cocaine (psychostimulant) Benzodiaze pines in the brain. |
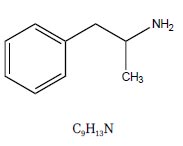 C9H13N |
| Cocaine (psychostimulant) | Benzodiazepines (98) | Oral, inhaled (used by mouth mostly) | Do not misuse medical care | 90% of the participants exhibited paranoid delusions, while 96% reported experiencing hallucinations, paranoia, and suspicious beliefs. | Psychostimulants, in the traditional sense, mainly focus on the monoaminergic systems, resulting in elevated levels of SER, DA, and/or NA in the extracellular space. |
 C17H21NO4 |
| Kratom | Naloxone | commonly used by chewing, as a tea, powdered in capsules and pills, or extracted for use in liquids | Medical care | - | - |
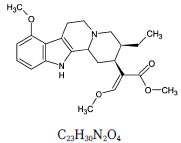 C23H30N2O4 |
| Hallucinogens (Tryptamines) | Naloxone | Inhalation, Intravenous, Oral |
The main chemical is in a kind of mushroom, so do not misuse | Perception will be interrupted, and alteration in the perception, spontaneous reoccurrence of perceptual disturbance, and the illusion of movement will exist. | All three subgroups share a common mechanism in the serotonergic system, represented by the agonism/partial agonism at the 5-HT2A receptor (activation), 5-HT1A, and 5-HT2C. However, Various hallucinogenic/psychedelic substances might have distinct interactions with various neurotransmitters, such as NMDA receptors, σ-receptors, μ-opioid receptors, and muscarinic receptors, in addition to their ability to inhibit serotonin and dopamine reuptake at their respective transporters. |
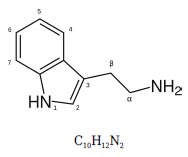 C10H12N2 |
| Phencyclidine | Diazepam, haloperidol, chlorpromazine |
Smoking, by mouth, snort, injection. |
Medical care | PCP exhibits more intense psychotic effects, such as hallucination and delusion, especially illogical thinking (79). Apathy (lack of interest), decreased talking, repetitive speech, and catatonic posturing (unusual body movements). |
- |
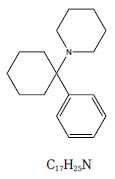 C17H25N |
| Entactogens, (MDMA) | Medical care | delusions (96%), hallucinations (96%), disorganization (96%). Feeling down (90%) with reduced emotional expression (81%), (77). |
- | - | - |
 C11H15NO2 |
| Antibiotics | Use them in a limited amount. | - | - | - | - | - |
3.6. Amphetamine
Amphetamine is a strong central nervous system stimulant. Amphetamines, such as methamphetamine and 3,4-methylenedioxymethamphetamine (MDMA), belong to a class of compounds called phenethylamines that induce catecholaminergic effects in the CNS and peripheral circulation. Nowadays, amphetamines are clinically used to treat short-term obesity, narcolepsy, and attention deficit disorder with hyperactivity [22]. Due to recent studies, psychosis following amphetamine use is characterized by delusions, visual hallucinations, and symptoms resembling acute psychosis most commonly observed in schizophrenia. There is an obvious pattern of high dosage and daily usage correlating with higher risks of substance-induced psychosis. Amphetamines impair the cognitive thought process and precede acute psychosis. This shows that continued impairment due to amphetamine use is a precursor to psychosis. (Table 3) [23, 24].
3.7. Cocaine
Cocaine is one of the most common substances that leads to transitory paranoia [25]. Cocaine is widely recognized to be associated with several mental disorders, and its use develops psychotic symptoms. Coke works as an inhibitor of serotonin and noradrenaline reuptake. The majority of psychotic symptoms are related to cocaine use within 24-48 hours [26, 27]. In sum, it is one of the most favorite drugs among teenagers and can be a serious risk factor and increase the possibility of psychoses in the future [28, 29] (Table 3).
3.8. Kratom
Kratom (Mitragyna speciose) is a psychoactive plant preparation that has medicinally been used for its stimulant effects and as an opioid substitute [30]. It can cause psychosis and even death. But the difference is that kratom’s effect for causing psychosis is stronger than other opioids. It can lead to addiction, sleeping and eating disorders as well. Also, neuropsychiatric side effects such as hallucinations, delusions and paranoia are usual after kratom intake [31] (Table 3).
3.9. Cathinone
Cathinone is related to the phenethylamine family but its potency is much lower than others [32]. It starts to have effects on consumers within 15 minutes at least and 45 minutes at most after injection. By inhaling, the sensations can be experienced within minutes and reach a higher intensity and stronger effect, but the effects last for 2-3 hours in oral and nasal use [33, 34]. This group consists of substances similar to the ones naturally occurring in Catha edulis (Khat) known as cathinone [35] (Table 3).
3.10. Hallucinogens
Hallucinogens include a wide group of natural and synthetic substances. As hallucinations are the intended toxidrome, these substances may cause psychosis. Currently, classic hallucinogens are seen as those that have a psychopharmacological profile similar to mescaline, psilocybin, and lysergic acid diethylamide (LSD) [36]. Classical hallucinogens (psychedelics) can be divided into three main chemical classes: tryptamines (e.g., psilocin), ergolines (e.g., LSD), and phenethylamines (e.g., mescaline). Tryptamines closely resemble serotonin chemically. Psilocybin and mescaline are natural, but LSD and LSD-like are synthetic drugs. It affects the visual cortex, which leads to illusions and open-eye dreams, which is one of the most important psychotic symptoms ref. There are two kinds of perception disorders by using hallucinogens: short-term, in which users do not experience significant impairment; psychiatric care is rarely sought; and long-term, which reflects chronic severe syndrome [37, 38] (Table 3).
3.11. Phencyclidine and Ketamine
These effects can be attributed to dopamine level incretion in the prefrontal cortex, which can be understood by considering the binding of ketamine and PCP to the dopamine receptor 2 (D2) [[39, 40]. Beck and coworkers discovered a noteworthy increase in temporary mental health issues related to ketamine usage [38, 41-43] (Table 3).
3.12. Antibiotics
Surprisingly, some kinds of antibiotics can lead to psychotic disorders (e.g., fluoroquinolones) [44-47] (Table 3).
3.13. Miscellaneous Compounds
Although, these are not the only substances that may lead to psychosis. There are other substances that can lead to psychosis; Dissociative, Sedatives or analgesics, New synthetic opioids (NSOs) (e.g., U-47700, U-49900, AH-7921, U-50488, U-51754, MT-45, Acetylfentanyl, Carfentanyl, Furanylfentanyl) [48], Desomorphine (‘krokodil’), Mitragynine (‘Kratom’, ‘kakuam’, ‘thang’, ‘ketum’, ‘biak’) [49], Salvinorin A (Salvia divinorum, hierba de Maria’, ‘Maria pastora’, ‘Sally-D’, ‘magic mint’) [50], Ketamine-like dissociatives; Ketamine (‘ket’, ‘special K’, ‘super K’, ‘kit-kat’) [51], Phencyclidine (PCP, ‘angel dust’, ‘supergrass’, ‘boat’) and PCP-type substances (e.g., 3- MeO-PCE, 4-MeO-PCP) [52], Methoxetamine (‘mexxy’, ‘special M’), Novel Stimulants and novel psychedelics [53];Synthetic cathinones (e.g., mephedrone, ‘m-cat’; ‘meow’) [54], Psychedelic/empathogenic phenethylamines (e.g., 2C series; D series, such as DOI, DOC; benzodifurans, such as ‘bromodragonfly’; others, such as PMA/PMMA) [55], Piperazines (e.g., BZP, mCPP, ‘party pills’, ‘smileys’) [56], Tryptamines (e.g., DMT, 5- MeO-DMT, ‘magic mushrooms’), Prescription drugs with a misusing potential: 1. ANTIDEPRESSANTS;(Bupropion, Amitriptyline, Venlafaxine (‘baby ecstasy’)) [57], 2. ANTIPSYCHOTICS: (Quetiapine (‘Susie Q,’ ‘Quell,’ and ‘baby heroin’); ‘Q ball’ (quetiapine with cocaine); ‘MaQ ball’ (quetiapine and marijuana), Olanzapine (‘Lilly’)) [58], 3. GABAPENTINOIDS (pregabalin and gabapentin), 4. Z-DRUGS (zaleplon, zolpidem and zopiclone) [59], DESIGNER BENZODIAZEPINES (e.g., clonazolam, etizolam, flubromazepam, phenazepam (‘Zinnie’) and pyrazolam [60], 5. OVER-THE-COUNTER DRUGS: (Codeine [61] (‘Purple drank’ is a mix of codeine and promethazine), Loperamide [62], Dextromethorphan (DXM) [63] for instance [64-72] (Tables 3 and 4).
| Medical Section | Category (type) |
|---|---|
| Psychoactive Substances | Alcohol Withdrawal and Hallucinosis, Amphetamine Intoxication, Cocaine Intoxication, Hallucinogen Intoxication, Phencyclidine Intoxication, Sedative Hypnotic Withdrawal |
| Cardiology | Digitalis, Beta-blockers, Antiarrhythmics |
| Oncology | Asparaginase, Cytarabine, Fluorouracil, Ifosfamide, Methotrexate, Vincristine |
| Infectious diseases | Ciprofloxacin, Antitubercular agents, Antimalarials, Antivirals |
| Neurology | Dopamine agonists (amantadine, bromocriptine, and levodopa) |
| Psychiatry | Antidepressants (bupropion, tricyclic antidepressants), Anticholinergics (benztropine, diphenhydramine) |
| Gastroenterology | Cimetidine, Ranitidine |
| Analgesia | Pentazocine, Meperidine, Indomethacin |
| Genera | Corticosteroids, Metrizamide, Methysergide, Baclofen Ephedrine |
4. DISCUSSION
In the last two decades, plenty of research has been dedicated to psychosis induced by cannabinoids, psychostimulants such as methamphetamine, amphe- tamine, methylphenidate and cocaine, hallucinogens and so on. Despite the apparent connection to psychotic symptoms, the scientific community is still unable to give definitive proof on this specific subject. The main point about the subject is that there has been a notable rise in both the quantity and diversity of newly developed psychoactive drugs. Over time, more powerful have been formulated and circulated, resulting in more harmful side effects and more severe impacts on the body. This surge in new drug misuse has greatly expanded the occurrence of secondary psychoses.
For example, synthetic cannabinoids and synthetic cathinone may lead to serious clinical syndrome with a high risk of a fully structured psychotic disorder [73, 74]. Clinicians still face a difficult task in differentiating SIP and primary psychotic illnesses. Nonetheless, we hold optimistic expectations that this research could assist in overcoming the challenge [75, 76].
But despite considerable variation in how substance exposure and psychosis were elicited or defined, there is a notable consistency across the population groups studied in different research. As has been said before, young ages play a big role in drug abuse. The most common reasons are fun or parents’ attitudes. On the other hand, drug abuse may have real side effects on the body and especially the brain as time passes and may lead to psychosis in the future. Although none of these variables, alone or together, can recognize the etiology of psychosis accurately. A combination of approaches is the best management for substance-induced psychosis, which includes medication management, psychological treatment (individual therapy or group therapy), and family engagement in some cases. After all, we have collected as much information as we could about different drugs that may lead to psychosis, psychotic symptoms, and similarities and differences between such substances. Finally, this article has been based on limited evidence, and further study of both pharmacologic and psychological interventions is needed to find out how to provide the best care to vulnerable youth and adults who have experienced such symptoms of psychosis and substance use. Systematic literature reviews are crucial in research articles for several reasons. For example, they provide a comprehensive overview of existing research on a particular topic, helping researchers understand the current state of knowledge. By following a systematic approach, researchers can ensure that the review is unbiased and based on all available evidence, reducing the risk of cherry-picking data. Systematic reviews help identify gaps in the existing literature, highlighting areas where further research is needed. They allow for the evaluation of the quality of individual studies, helping to assess the reliability of the findings. Also, systematic reviews can facilitate meta-analysis, where data from multiple studies are combined to provide more robust conclusions. The results of systematic reviews can inform policy-making, clinical practice, and future research directions. Overall, using systematic literature reviews in articles enhances the credibility and reliability of the research by providing a structured and rigorous synthesis of existing knowledge. The research includes most of the substances that can lead to psychoses, and it is a comprehensive article that can help to identify these substances conveniently. Psychoactive substances and some medications can cause secondary psychosis. For example, Digitalis, Beta-blockers, Antiarrhythmic in cardiology, Asparaginase, Cytarabine, Fluorouracil, Ifosfamide, Methotrexate, Vincristine in oncology, Dopamine agonists (amantadine, bromocriptine, and levodopa) in neurology, Cimetidine, Ranitidine in gastroenterology and Antidepressants (bupropion, tricyclic antidepressants), Anticholinergics (benztropine, diphenhydramine) in psychiatry can cause secondary psychosis (Table 4).
5. LIMITATIONS AND FUTURE DIRECTIONS
This systematic review has some limitations. There are few scientific research and articles about substance-induced psychoses, and it is difficult to say with certainty that these substances lead to psychoses definitely, and these are all of the substances that may lead to psychoses. First of all, this article has been written about humans, and there is nothing certain about humans, and the effects of substances differ from one another. Secondly, there are lots of substances that are undetermined and uncharted. Also, there will be more human-made substances in the future. Further studies and investigations are required to verify these substances and to find antidotes and cures for substance-induced psychotic patients as well. Finally, this research can only represent the situation of a single part of the whole world population.
CONCLUSION
A few studies indicate that there are a few substances and even medicines that may lead to psychoses with high possibility. Numerous psychological intervention strategies for SIPs show promising treatment results, indicating the potential for customizable interventions that can meet individual needs. It can be concluded that the etiology of psychoses is different. Psychoses can develop because of sad experiences in childhood, available genes, depressing experiences and accidents, some medicines for a long time, or drug misuse. However, the most common reasons are available genes and substances that have been discussed. Unfortunately, these substances change the chemical structures of genes and can lead to other disorders and diseases besides psychoses. However, additional research is needed to effectively put these strategies into practice in interventions that are supported by a reliable mechanism of change and to verify the effectiveness of those interventions.
AUTHORS' CONTRIBUTIONS
Research design: Isaac Karimi
Data collection: Nioosha Pooyanmehr
Writing the manuscript: Nioosha Pooyanmehr
Primary revision: Isaac Karimi

